Arrhythmias - Atrial fibrillation (Afib): Nursing
Arrhythmias - Atrial fibrillation (Afib): Nursing
Acute Final
Acute Final
Notes
| ARRHYTHMIAS - ATRIAL FIBRILLATION (AFIB) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Atrial fibrillation, sometimes called Afib for short, is the most common cardiac arrhythmia which occurs when the atria contract way faster than normal, and in a disorganized manner. As a result, the atria have a quivering, or twitching movement that can’t pump blood into the ventricles efficiently.
Now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atrium, creating the P wave on an ECG. And when the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles.
From the atrium, electrical activity goes to the atrioventricular, or AV node, where impulse propagation speed slows way down; this is the PR interval on an ECG. This pause allows the atria to contract while the ventricles fill with blood.
From the AV node, the depolarization wave goes through the Bundle of His, then the right and left branches of the Bundle, and finally through the Purkinje fibers, which deliver the current to the right and left ventricles, causing them to depolarize. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations, and it’s represented by the QRS complex on an ECG.
Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the pause between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Okay, now, atrial fibrillation is typically caused by any kind of structural damage to the heart, or any damage to the electrical conduction system of the heart. Often, these changes are strongly associated with several cardiovascular disorders and a variety of risk factors. For example, high blood pressure, coronary artery disease, valvular diseases, essentially anything that can create an inflammatory state or physically stretches the atria, may potentially damage the cells in the atria and lead to atrial fibrillation.
Other risk factors include non-modifiable risk factors like being assigned male at birth, aging, and a personal or family history of heart disease or atrial fibrillation; as well modifiable risk factors like obesity, diabetes, stroke, thyrotoxicosis, which means excess levels of thyroid hormones; excessive caffeine use, meaning more than 4 cups a day; stress, and excessive alcohol consumption.
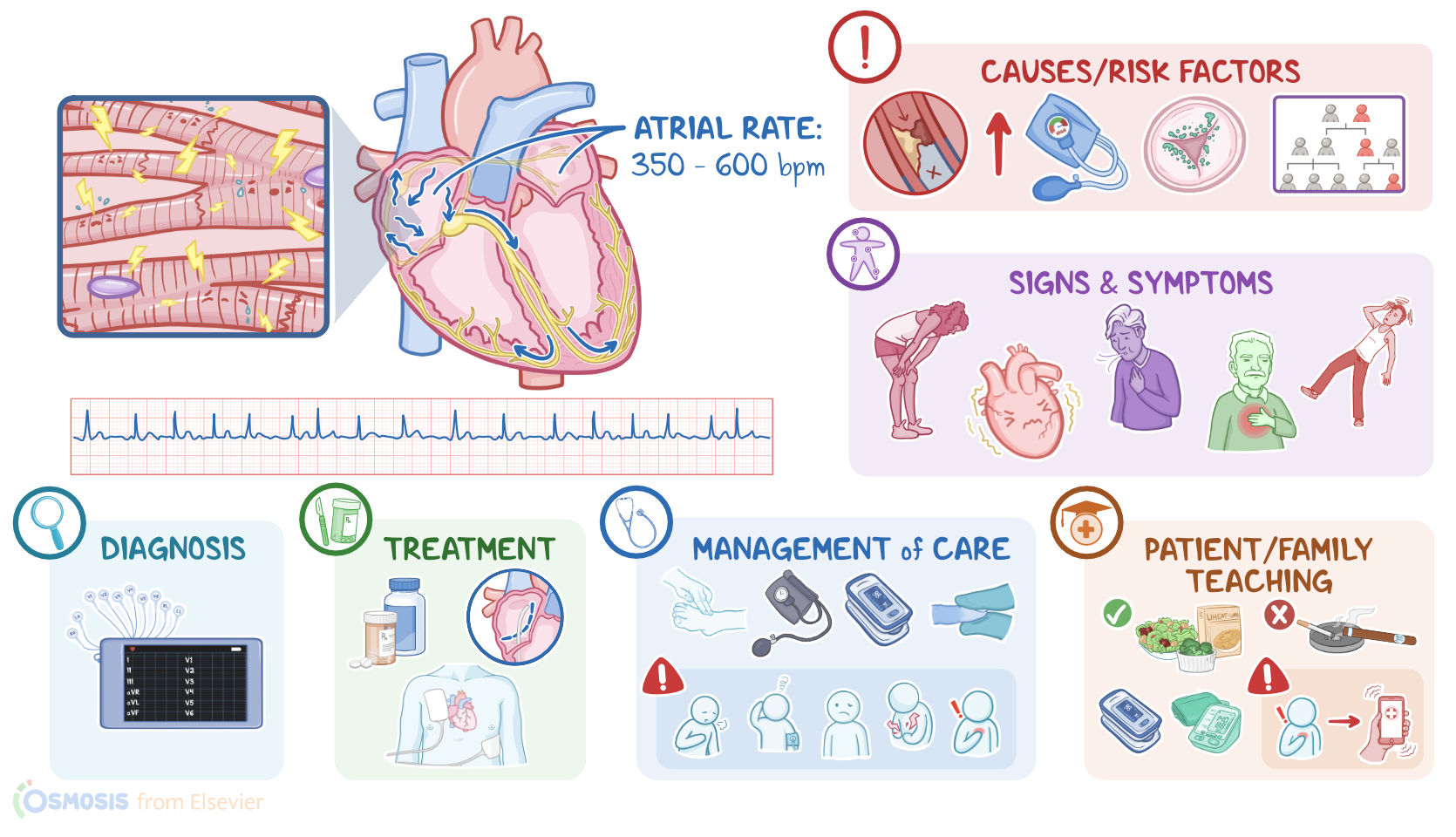
These factors likely stress and damage the cells in the atria, which can lead to tissue heterogeneity; or in other words, cells start taking on different electrical properties, and end up generating impulses from many foci in a totally disorganized manner, that tends to override the sinoatrial node. So instead of one efficient atrial contraction, clients get all these mini contractions, usually between 350 and 600 per minute, that make it look like the atria are just quivering.
Sometimes, signals from one of these areas make it down to the ventricles and cause irregular ventricular contraction; these QRS complexes are interspersed at irregular intervals though, and usually at fairly high rates, between 100 and 150 beats per minute. As a result, ventricular filling is also impaired, which reduces cardiac output.
Additionally, the inefficient emptying of the atria into the ventricles can cause blood to stay in the atria for longer than normal, so it can form atrial clots. So with atrial fibrillation, there’s a chance that one of these clots can get pumped from the atria into the ventricles, and from there, into the circulation. From there, the clot can get lodged in a cerebral artery, causing a stroke; in a pulmonary artery branch, causing a pulmonary embolism; or in a coronary artery that supplies the myocardial muscle, causing a myocardial infarction.
Oftentimes, people with atrial fibrillation start by experiencing paroxysmal events, which means AFib suddenly comes and goes, lasting less than a week at a time, probably because the tissue is still relatively healthy. Repeated paroxysmal events that occur over longer periods of time tend to stress the atrial cells even more. Over time, the cells in the atrium undergo progressive fibrosis or scarring, which means the AFib episodes didn’t terminate spontaneously in less than a week. AFib episodes that last longer than one week are called persistent AFib, and when it lasts for more than 12 months, then it’s called long-standing persistent AFib. Finally, when long-standing persistent AFib is left untreated or doesn’t respond to treatment, that’s called permanent atrial fibrillation; and in time, it can lead to heart failure.
Now, the clinical manifestations of atrial fibrillation include general fatigue, dizziness, shortness of breath, exercise intolerance, anxiety, and weakness. Clients might also describe palpitations or thumping in their chest. On auscultation, fast, irregular heart beats can be heard; and since the atria don’t contract efficiently, the S4 sound can’t be heard.
Additionally, if a clot leaves the heart and gets lodged in another artery, manifestations depend on where the clot lands. With a stroke, there could be confusion, slurred speech, and unilateral weakness or paralysis of the face or limbs; with a pulmonary embolism, there might be dyspnea and chest pain; and with a myocardial infarction, there could be severe chest pain that radiates, most commonly to the left arm.
Diagnosis of atrial fibrillation starts with the client’s history and physical assessment. The next step is a 12 lead ECG, which shows an irregular rhythm, and an atrial rate as high as 350 to 600 beats per minute with chaotic and fibrillatory waves that replace the normal P waves. As a consequence, the PR interval is not measurable. Ventricular rate usually varies, but can reach 150 beats per minute. However, the QRS complexes usually look normal. The ventricular rate in AFib with controlled ventricular response is between 60 to 100 beats per minute, but can go higher than 100 beats per minute if the response is uncontrolled. A common presentation is 2:1 conduction with an atrial rate of 300 beats per minute and a ventricular rate of 150 beats per minute. Additionally, a transthoracic echocardiogram can be done to evaluate the overall morphology of the heart, while a transesophageal echocardiogram, or TEE, can be done to evaluate for clots in the atrium.