Arterial blood gas (ABG) - Metabolic acidosis: Nursing
1,830views
Arterial blood gas (ABG) - Metabolic acidosis: Nursing
487 Final
487 Final
Notes
| ARTERIAL BLOOD GAS (ABG) - METABOLIC ACIDOSIS | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INTERPRETATION |
| |
| MANAGEMENT OF CARE |
| |
Transcript
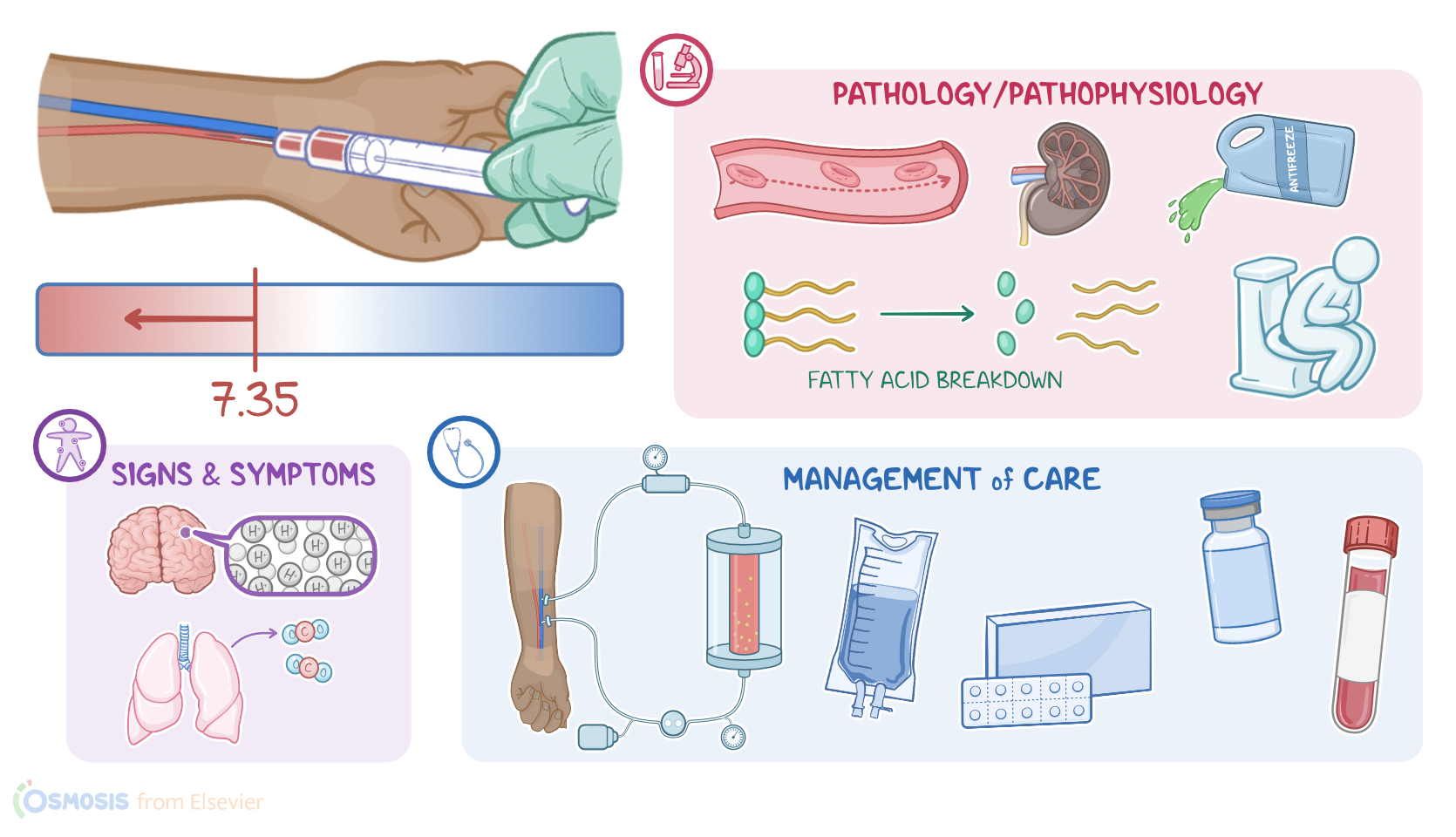
A 55-year-old client with a history of type 1 diabetes mellitus is brought to the emergency department with a sudden onset of confusion. On assessment, her mucous membranes are dry; and she is tachycardic, hypotensive, and her respirations are deep and fast. The healthcare provider suspects metabolic acidosis secondary to diabetic ketoacidosis so, an arterial blood gas is ordered to assess for changes in acid-base balance.
So arterial blood gas, or ABG for short, is a test used to measure the acid-base components and pressure of gasses in the arterial blood. Normal ABG values for healthy adults are a pH ranging from 7.35 to 7.45, bicarbonate, or HCO3- ranging from 21 to 28 mEq/L; carbon dioxide or PaCO2 ranging from 35 to 45 mm Hg; PaO2 ranging from 80 to 100 mm Hg, and SaO2 should be more than 95%.
Okay, there are four major ways excess acid can accumulate in the body. The first way is when there’s increased acid production, like with lactic acidosis, which is caused by decreased tissue perfusion and resulting anaerobic metabolism, or with diabetic ketoacidosis, which involves extreme hyperglycemia and an excessive breakdown of fatty acids in people with diabetes. It can also be caused by increased ingestion of acids, like methanol, salicylates, or ethylene or propylene glycol.
Then there’s decreased elimination of acids, which can happen with renal failure; and finally increased elimination of base, like with excessive diarrhea, which eliminates too much HCO3- from the intestines.
You can easily remember causes of metabolic acidosis by using the mnemonic MUDPILES, where M stands for methanol; U for uremia, which happens in renal failure; D for diabetic ketoacidosis, P for propylene glycol; I for iron tablets and isoniazid, which can cause acidosis with an overdose; L for lactic acidosis; E for ethylene glycol; and finally, S for salicylates.
Now, as the pH continues to decrease and move out of the normal range, the body will attempt to correct the imbalance, a process called compensation. With metabolic acidosis, the respiratory system is the main mode of compensation. The process begins when chemoreceptors in the brain sense a high concentration of hydrogen ions, which stimulates an increase in respirations, or hyperventilation, which increases the rate at which CO2 is eliminated from the body. For example, if the underlying cause is diabetic ketoacidosis, Kussmaul respirations, or rapid, deep respirations will be present. Compensation can't completely correct the pH imbalance, and it won’t fix the underlying cause of it either
To interpret an ABG, the first thing you’ll do is to look at the pH. If it’s less than 7.35 your client is acidotic; and if it’s greater than 7.45 your client is alkalotic.
Once you know whether your client is acidotic or alkalotic, you’ll look at the PaCO2 and HCO3- and compare it to the pH to determine if the acid-base imbalance is caused by a metabolic or a respiratory issue. When an acid-base imbalance is primarily caused by a respiratory issue, the pH and PaCO2 will move in the opposite direction; so, as the pH increases, the PaCO2 decreases, and vice versa.
On the other hand, when an acid-base imbalance is primarily caused by a metabolic issue, the pH and HCO3- will move in the same direction. So, as the pH increases, the HCO3- also increases, and vice versa. You can use the ROME acronym to help you remember these relationships, where RO stands for Respiratory and Opposite for the relationship of pH and PaCO2, and ME stands for Metabolic and Equal for the pH and HCO3- relationship.