Arterial blood gas (ABG) - Overview: Nursing
2,708views
Arterial blood gas (ABG) - Overview: Nursing
371
371
Notes
| ARTERIAL BLOOD GAS (ABG) - OVERVIEW | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
Transcript
Arterial blood gas, or ABG for short, is a test used to measure the acid-base components and pressure of gasses in the arterial blood.
Now, the components of an ABG are pH, bicarbonate, carbon dioxide, and oxygen. First, there’s pH which reflects the concentration of hydrogen ions, or H+, in the blood.
There’s an inverse relationship between pH and H+, meaning that when there’s more H+, the pH decreases and becomes more acidic, and, when there’s less H+, the pH increases, and becomes less acidic. The normal pH ranges from 7.35 to 7.45. If the pH is less than 7.35, it's considered acidosis; while a pH greater than 7.45 is alkalosis.
Then, there’s bicarbonate, HCO3-, which is a base: a substance that can combine with H+ and remove it from solution. When there’s more HCO3-, the pH increases and becomes more basic, and, when there’s less HCO3-, the pH decreases, and becomes more acidic. Normally, HCO3- ranges from 21 to 28 mEq/L.
Up next is the partial pressure of carbon dioxide, or PaCO2, which measures the amount of carbon dioxide dissolved in the arterial blood; and partial pressure of oxygen, or PaO2, which measures the amount of oxygen in the arterial blood. For these gasses, “P” stands for partial pressure and “a'' stands for arterial. The normal PaCO2 should range from 35 to 45mm Hg, and PaO2 should range from 80 to 100mmHg.
Finally, there’s oxygen saturation or SaO2, which refers to the percentage of hemoglobin molecules in the blood that have oxygen attached to them. SaO2 should be 95% or more.
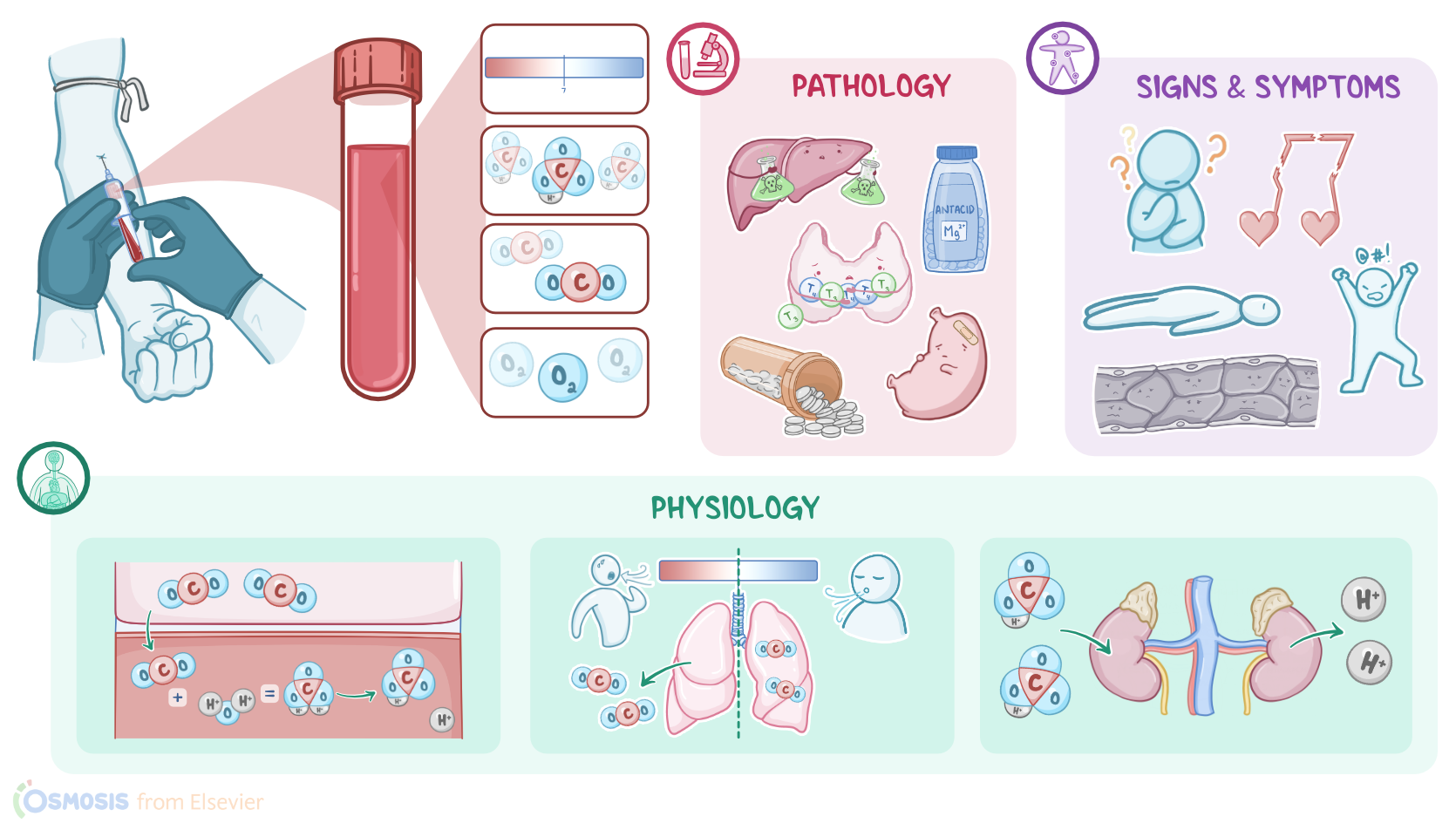
Now, when you think about it, acids are continually being produced by normal metabolic processes like cellular oxidation and the breakdown of nutrients, so the body needs a way to handle all these hydrogen ions to prevent major shifts in the overall pH. To accomplish this, the body has three lines of defense to help maintain an optimal pH: the cellular buffering system, the lungs, and the kidneys.
The first line of defense is the cellular buffering system. Now, in everyday language a buffer is something that acts like a protective cushion, and the same is true of physiologic buffers; they protect the pH balance by keeping it from rising or falling too quickly. This system is always present and responds within seconds when there’s a disturbance in the pH. The most common buffer in the body is the bicarbonate-carbonic acid system.
It all starts with a by-product of cell metabolism called carbon dioxide or CO2, which is released by the cells into the blood. In the blood, CO2 mixes with water, or H2O, to form carbonic acid, or H2CO3. Now, carbonic acid easily dissociates into bicarbonate, and hydrogen ions. This reaction can go in both directions, which is actually how the buffering system works.
Now, if the pH is increased, which means that there is less H+, we call that alkalosis. To oppose alkalosis, this reaction is amplified and we get more bicarbonate and hydrogen ions. In contrast, decreased pH, which means there is more H+, is called acidosis. To oppose acidosis, the reaction is reversed. So, excess H+ are used by bicarbonate to generate more carbonic acid, which gives us more carbon dioxide that can be eliminated by the lungs.
So, the lungs are the second line of defense, which respond to shifts in pH by changing the respiration rate. With acidosis, chemoreceptors in the brain sense a high concentration of hydrogen ions, and stimulates an increase in respirations so more CO2 is eliminated from the body. Alternatively with alkalosis, chemoreceptors sense a low concentration of hydrogen ions, and stimulate a decrease in the respiratory rate so more CO2 is retained. This is a quick response, occurring within minutes of acid-base alterations.
For the last line of defense, we have the kidneys, which help maintain pH by eliminating excess H+ and reabsorbing more bicarbonate. This is a slow response, which can take hours to days.