Arterial blood gas (ABG) - Respiratory acidosis: Nursing
1,445views
Notes
| ARTERIAL BLOOD GAS (ABG) - RESPIRATORY ACIDOSIS | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INTERPRETATION |
| |
| NURSING IMPLICATIONS |
| |
Transcript
A 75-year-old male client with a history of end-stage chronic obstructive pulmonary disease, or COPD, is brought to the emergency department with shortness of breath and disorientation. On assessment, he is tachypneic; cyanotic around his lips and earlobes; and respirations are rapid and shallow. The health care provider suspects respiratory acidosis secondary to end-stage COPD exacerbation, so an arterial blood gas is ordered to assess for changes in acid-base balance.
Alright, arterial blood gas, or ABG for short, is a test used to measure the acid-base components and pressure of gasses in the arterial blood. Normal ABG values for healthy adults are a pH ranging from 7.35 to 7.45, bicarbonate, or HCO3- ranging from 21 to 28 mEq/L; carbon dioxide or PaCO2 ranging from 35 to 45 mm Hg; PaO2 ranging from 80 to 100 mm Hg, and SaO2 should be more than 95%.
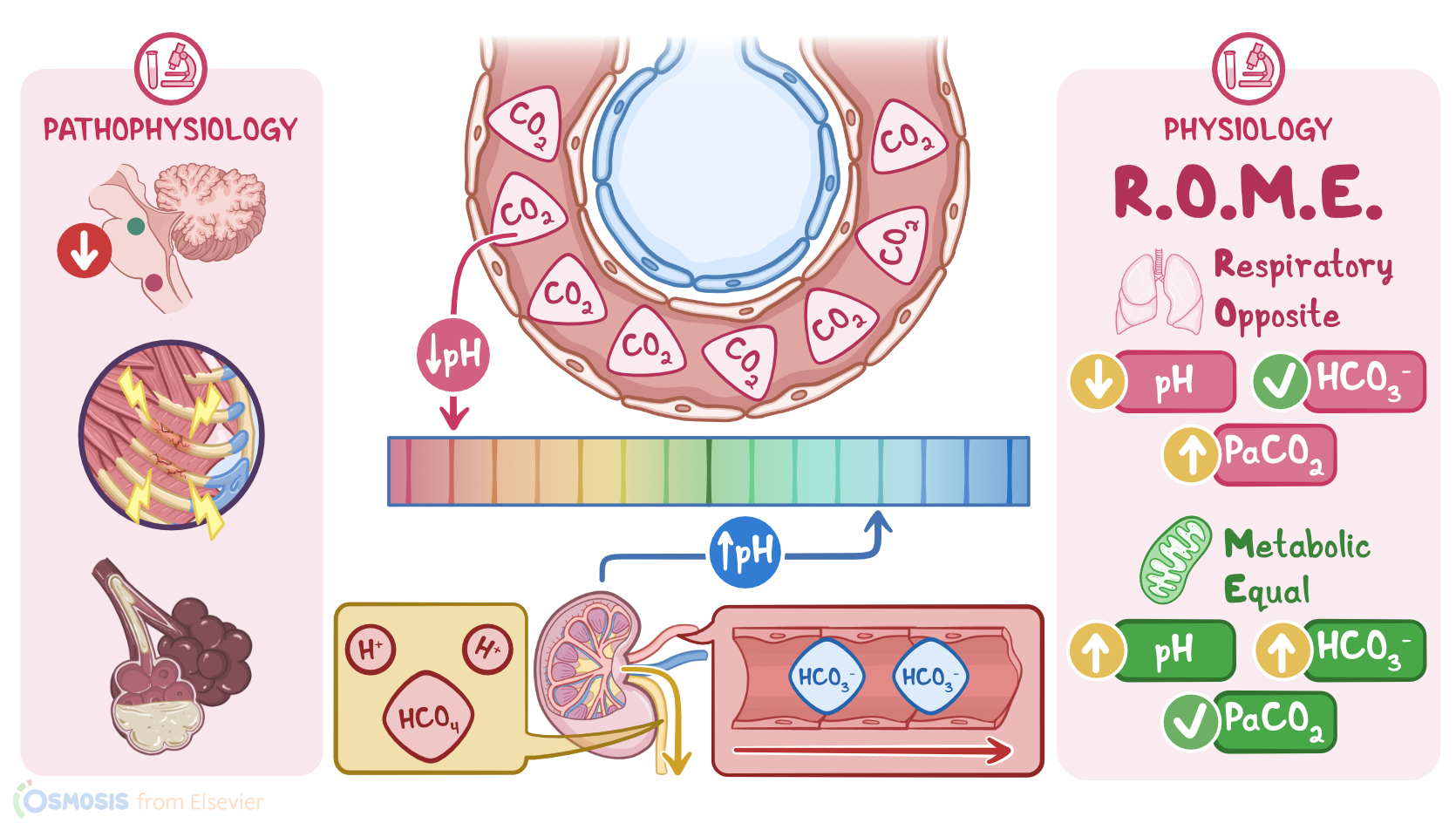
Now, respiratory acidosis is a condition in which the normal mechanism of ventilation is disturbed, resulting in hypoventilation. During hypoventilation, the respiratory rate and depth both decrease, the minute ventilation, which is the volume of air that moves in and out of the lungs in a minute, decreases, and the amount of CO2 eliminated from the body decreases.
So, more CO2 is retained because there's more CO2 produced by the body than can be eliminated. In the blood, increased CO2 binds to water, and forms carbonic acid, which then dissociates into hydrogen ions, and bicarbonate. Initially, the increase in bicarbonate helps buffer the hydrogen ions, slowing the drop in pH. Over time, the increased amount of hydrogen will eventually result in acidosis.
Now, there are some conditions that can alter ventilation, including those that can affect the respiratory center in the brain, as well as the lungs, the respiratory muscles, or gas exchange itself. For example, a stroke and medications like opiates and barbiturates depress the respiratory center in the brain, slowing respirations and increasing the risk of hypoventilation.
Sometimes, the lungs can’t ventilate properly, like when there is an airway obstruction that prevents air from entering or exiting the lungs. Then, with chest trauma, ventilation can be decreased due to pain. Finally, in other conditions, like COPD and pulmonary edema, the lungs and muscles work properly, but the gas exchange is reduced.
Now, as the pH continues to decrease and move out of the normal range, the body will attempt to correct the imbalance, a process called compensation. With respiratory acidosis, the renal system is the main mode of compensation. The process begins when the kidneys start to excrete the excess acid, while also reabsorbing bicarbonate. Compensation can't completely correct the pH imbalance, and it won’t fix the underlying cause of the pH imbalance.
Clinical manifestations of respiratory acidocis can initially include headache and restlessness, followed by lethargy, myocardial depression, and hypotension. Skin and mucous membranes can remain pink from CO2-related vasodilation, or cyanotic if hypoxemia is present.
To interpret an ABG, the first thing you’ll do is to look at the pH. If it’s less than 7.35 your client is acidotic; and if it’s greater than 7.45 your client is alkalotic. Once you know whether your client is acidotic or alkalotic, then you’ll look at the PaCO2 and HCO3- and compare it to the pH to determine if the acid-base imbalance is caused by a metabolic or a respiratory issue.
Sources
- "Saunders Nursing Guide to Diagnostic and Laboratory Tests - E-Book" Elsevier Health Sciences (2011)
- "Laboratory Tests and Diagnostic Procedures with Nursing Diagnoses" Pearson (2018)
- "Respiratory Acidosis" StatPearls (2022)
- "Saunders comprehensive review for the NCLEX-RN® examination" Elsevier (2020)
- "Mosby’s Diagnostic and Laboratory Test Reference" Elsevier (2021)