Arterial blood gas (ABG) - Respiratory alkalosis: Nursing
1,055views
Arterial blood gas (ABG) - Respiratory alkalosis: Nursing
NURS 223 fa23 Week 2 - Acid/Base Balance and Disorders (must be watched by lecture on 8/31, try to watch earlier as we may start this content on 8/28)
NURS 223 fa23 Week 2 - Acid/Base Balance and Disorders (must be watched by lecture on 8/31, try to watch earlier as we may start this content on 8/28)
Notes
| ARTERIAL BLOOD GAS (ABG) - RESPIRATORY ALKALOSIS | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INTERPRETATION |
| |
| MANAGEMENT OF CARE |
| |
Transcript
A 24-year-old female client arrives at the emergency department with a report of shortness of breath. She has a history of anxiety and was unable to pay for her medications this month. On assessment her lungs are clear, her heart rhythm is sinus tachycardia, and she is afebrile. Based on these findings, the health care provider suspects anxiety-induced hyperventilation so an arterial blood gas is ordered to assess for changes in the acid-base balance.
Alright, arterial blood gas, or ABG for short, is a test used to measure the acid-base components and pressure of gasses in the arterial blood. Normal ABG values for healthy adults are a pH ranging from 7.35 to 7.45, bicarbonate, or HCO3- ranging from 21 to 28 mEq/L; carbon dioxide or PaCO2 ranging from 35 to 45 mm Hg; PaO2 ranging from 80 to 100 mm Hg, and SaO2 should be more than 95%.
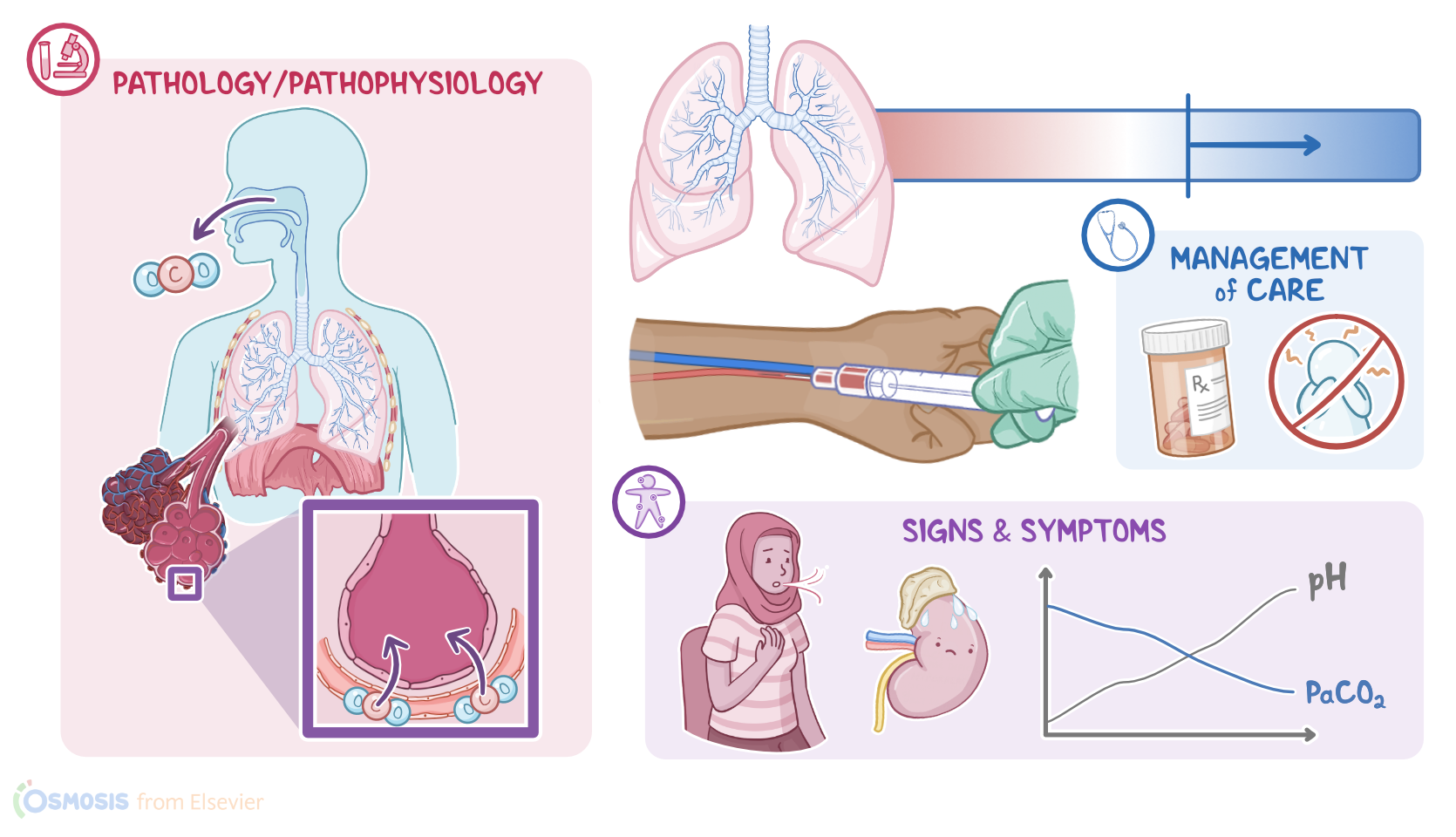
Now, respiratory alkalosis is a condition when increased pH is caused by hyperventilation due to central causes like head injury or by anxiety-induced hyperventilation; as well as pulmonary causes like pulmonary emboli; or iatrogenic causes like mechanical ventilation.
During hyperventilation, too much carbon dioxide, or CO2, is blown out by the lungs. Ultimately, more CO2 is removed from the body than what is created during normal cellular metabolism, leading to a hypocapnia, or low CO2.
Now, as the pH continues to increase and move out of the normal range, the body will attempt to correct the imbalance, a process called compensation. With respiratory alkalosis, the renal system is the main mode of compensation. The process begins when the kidneys decrease reabsorption of HCO3-, which decreases the pH. However, compensation can’t completely correct the pH imbalance, and it won’t fix the underlying cause of the pH imbalance.
Okay, to interpret an ABG, the first thing you’ll do is look at the pH. If it’s less than 7.35 your client is acidotic; and if it’s greater than 7.45 your client is alkalotic.
Once you know that you know whether your client is acidotic or alkalotic, you’ll look at the PaCO2 and HCO3- and compare it to the pH to determine if the acid-base imbalance is caused by a metabolic or a respiratory issue.
When an acid-base imbalance is primarily caused by a respiratory issue, the pH and PaCO2 will move in the opposite direction; so, as the pH increases, the PaCO2 decreases, and vice versa. On the other hand, when an acid-base imbalance is primarily caused by a metabolic issue, the pH and HCO3- will move in the same direction. So, as the pH increases, the HCO3- also increases, and vice versa.