Bladder tumors: Nursing
Bladder tumors: Nursing
Watch later
Watch later
Notes
| BLADDER TUMORS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATEMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Bladder tumors are growths arising from various tissue layers of the bladder wall. Malignant bladder tumors include urothelial carcinoma, which is the most common type, as well as squamous cell carcinoma and adenocarcinoma, among others, and these tumors can spread to surrounding tissues and organs.
In contrast, benign bladder tumors, including urothelial papilloma, leiomyoma, fibroma, and hemangioma, are less common, and stay localized to the bladder.
Okay, let’s quickly review some anatomy and physiology.
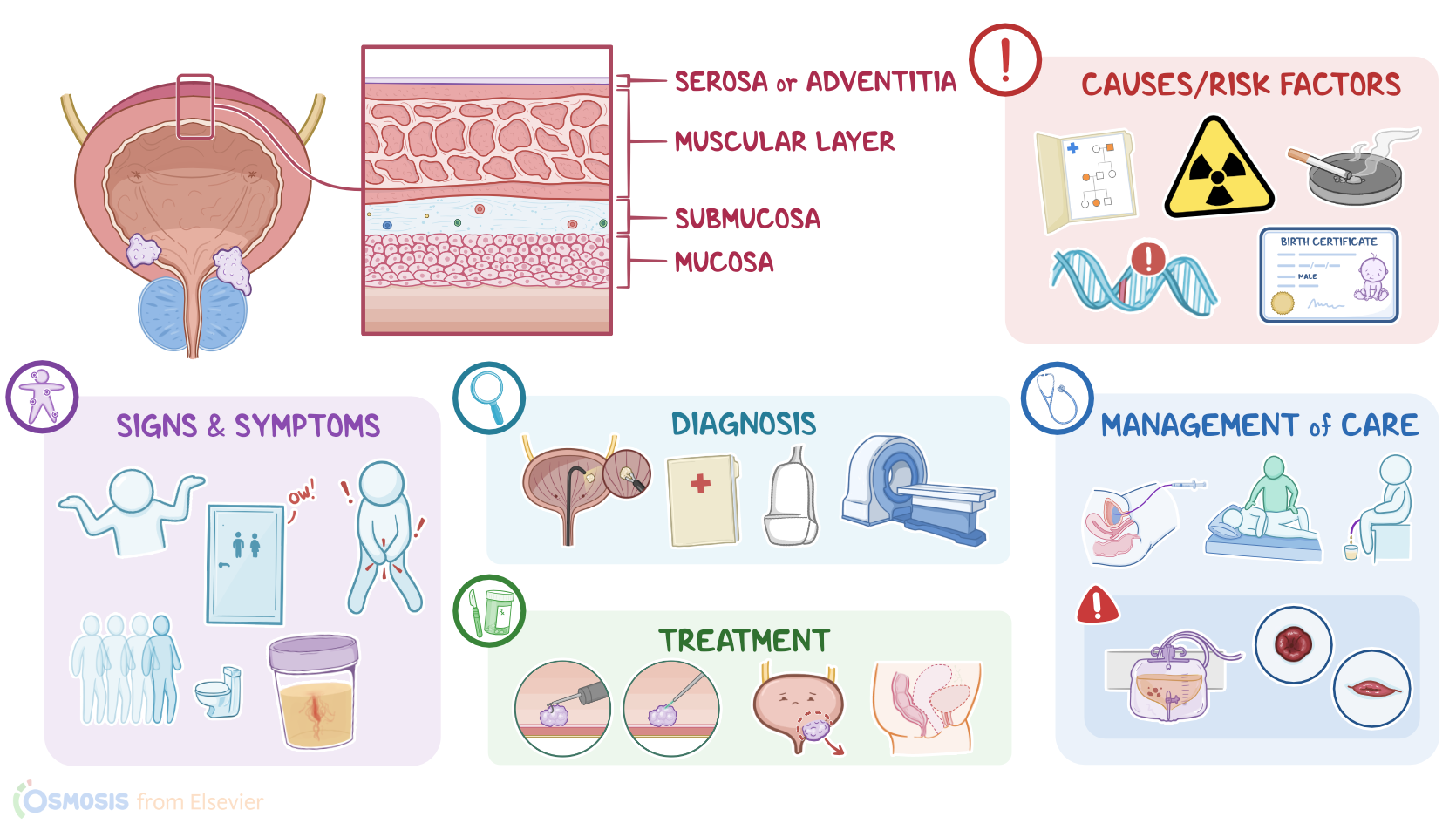
The urinary bladder is a hollow visceral organ that’s basically a reservoir for holding urine. Let's zoom into the wall of the urinary bladder which is made up of four layers. The outermost layer is called serosa, or adventitia. Next is the muscular layer, which contracts to allow urine to pass down into the urethra. After that is the submucosa, which consists of a dense layer of tissue that contains blood vessels, lymphatics, and nerves. And finally, there’s the innermost layer, called the mucosa, which consists of a special type of epithelial cells, called urothelial cells.
Now, the exact cause of bladder tumors is unknown, but there’s typically a genetic mutation in one of the cells of the bladder. These mutations may arise from a variety of risk factors. Nonmodifiable risk factors include age above 55 years, family history of bladder tumors, being assigned male at birth, and white race.
On the other hand, modifiable risk factors include exposure to toxic substances, most importantly tobacco use, or industrial dyes, radiation, medications like cyclophosphamide, as well as obesity. Damage to the bladder from chronic urinary tract infections or recurrent kidney stones also increases the risk for bladder tumors.
Okay, so the pathology of bladder tumors begins once a cell of the bladder wall becomes mutated and starts dividing uncontrollably, forming a tumor. The most common type of benign bladder tumor is urothelial papilloma, which arises from a urothelial cell, followed by tumors arising from other cell types, like leiomyoma which originate from the smooth muscle in the bladder wall, fibroma that develop from connective tissue, and hemangioma that grow from blood vessels.
Benign tumors tend to just grow as one papillary outgrowth into the bladder lumen as in urothelial papilloma or towards the outer wall like leiomyoma.
On the other hand, the most common type of malignant bladder tumor is urothelial carcinoma, which, again, arises from a urothelial cell, followed by squamous cell carcinoma and adenocarcinoma.Now, what makes things confusing is that both squamous cell carcinoma and adenocarcinoma also develop from urothelial cells.
Chronic inflammation or irritation can cause urothelial cells to change shape and take on the flat, pancake-like appearance of squamous cells, or the mucus filled glandular cells. This is called metaplasia and it’s still benign. When these cells start growing out of control, it becomes squamous cell carcinoma or adenocarcinoma.
Now, malignant tumors of the bladder may start as papillary outgrowth from the bladder mucosa and sometimes even grow horizontally. As the tumor keeps growing, it’ll start penetrating deeper into the bladder wall and new blood vessels also develop via angiogenesis to supply it.
Eventually, cancerous cells break through the wall and start invading neighboring tissues, like the prostate, rectum, and vagina and may even spread to nearby lymph nodes or metastasize to other organs, such as the lungs, liver, and bones.
Now, the clinical manifestations of bladder tumors vary based on the size and location of the tumor. Initially, clients can be completely asymptomatic.
Over time, as the tumor grows in size and invades deeper into the bladder, clients can start experiencing painless hematuria, which can be microscopic or gross. If the tumor grows enough to physically obstruct the urinary flow, it can cause pelvic pain, dysuria, and frequent and urgent urination. Sometimes a large bladder tumor can even be palpated in the lower abdomen.
Diagnosis of bladder tumors begins with the client’s history and physical assessment, followed by imaging tests, like a CT, MRI, or ultrasound, to visualize the tumor.
Diagnosis is then confirmed with cystOscopy with biopsy. This helps differentiate between benign and malignant tumors, as well as provide information about the tumor grading and staging.
Grading is based on how well the tumor cells resemble normal tissue which can range from well-differentiated, considered low-grade tumors, to undifferentiated, which are high-grade tumors, and are more likely to grow rapidly and metastasize.
Staging is then determined based on how far a tumor has already spread. A tumor at stage 1 is localized to the bladder mucosa. At stage 2 it has invaded the bladder wall. At stage 3 it has spread to surrounding tissue and organs like the prostate and uterus. And finally, stage 4 is when it has begun to spread by metastasizing into distant sites like the lymph nodes, lungs, bone, or liver.
Treatment for bladder tumors depends on their aggressiveness and extension. Small tumors that are localized to the bladder mucosa can be treated with a transurethral resection or laser ablation of the tumor. Clients with tumors that spread deeper into a single area of the bladder wall are treated with a partial cystectomy, which is when the affected part of the bladder is surgically removed.
On the other hand, for clients with larger tumors that have spread to the surrounding organs, the treatment of choice is radical cystectomy, or removal of the entire bladder, along with the nearby lymph nodes and surrounding organs, including the uterus, or the prostate glands. This surgical procedure is typically followed by additional procedures, called urinary diversions, that create alternative pathways for urine elimination.
Incontinent urinary diversions, such as an ileal conduit, result in a connection to a urinary collection bag outside the body. Alternatively, continent urinary diversions, like a Kock or Indiana pouch, or ileal neobladder create a storage pouch inside the body made from the small intestine. A valve is created for those with a Kock or Indiana pouch, through which the client inserts a catheter to drain the collection pouch. On the other hand, a neobladder is connected to the urethra so a client can control when urine leaves their body by relaxing their pelvic floor muscles and then bearing down with their abdominal muscles.
Alternatively, nonsurgical treatment options include intravesical chemotherapy, which means the medication is instilled into the bladder, as well as immunotherapy using Bacillus Calmette-Guérin or BCG applied directly to the bladder tumor in order to slow tumor growth. Now, for clients with unresectable metastatic tumors, as well as those who can’t have surgery, treatment can involve systemic chemotherapy or radiation therapy, as well as palliative care to decrease their symptoms and improve quality of life. Okay, let’s look at the nursing care you’ll provide to clients with a bladder tumor. Your priority nursing goals are to manage complications related to the treatment regimen, provide postoperative care, and provide psychosocial support.
If your client is prescribed intravesical therapy with BCG, begin by assisting them to completely empty their bladder.
Then, insert a urinary catheter and administer the medication.
After administration, assist your client to rotate their position every 15 minutes to increase the medication’s contact with the bladder surface.
After 2 hours, assist them to empty their bladder, ensuring they are in a sitting position to reduce the risk of splashing.
Then, provide fluids to help flush the remaining medication out of the bladder.
Report to the healthcare provider if your client shows signs of hemorrhagic cystitis, including passing blood clots or copious amounts of blood in the urine, and prepare them for bladder irrigation, blood product administration, or operative intervention as prescribed.