Case study - Delirium: Nursing
Notes
| CASE STUDY - DELIRIUM | ||
| KEY POINTS | NOTES | |
| INTRODUCTION |
| |
| RECOGNIZING AND ANALYZING CUES |
| |
| PRIORITIZING HYPOTHESES, GENERATING SOLUTIONS, AND TAKING ACTIONS |
| |
| EVALUATING OUTCOMES |
| |
Transcript
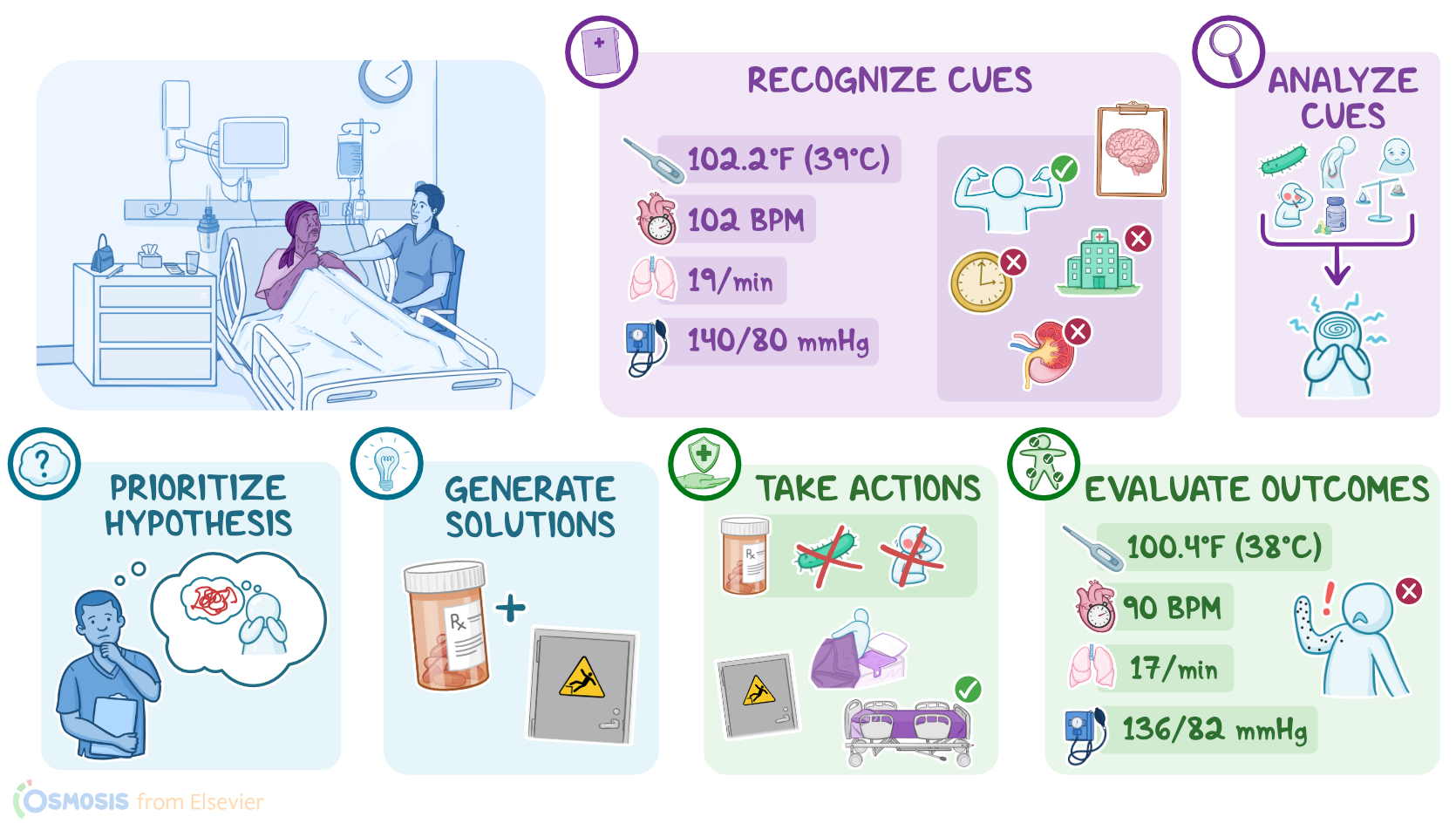
Nurse Melinda works on a medical surgical unit and is caring for Kadija, a 72-year-old with a history of heart failure who was admitted for pyelonephritis. After settling Kadija in her room, Nurse Melinda goes through the steps of the Clinical Judgment Measurement Model to make clinical decisions about Kadija’s care by recognizing and analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes.
First, Nurse Melinda recognizes important cues, including Kadija’s vital signs, which are temperature of 102.2 F or 39 C, heart rate 102 beats per minute, respirations 19 breaths per minute, and blood pressure 140/80 mmHg.
Nurse Melinda notices Kadija appears anxious, and her eyes are moving back and forth across the room. She gathers additional information from Kadija.
Nurse Melinda: Hi Kadija, how are you feeling today?
Kadija: Don’t you see that? There are a bunch of spiders on the wall behind you.
Nurse Melinda turns around and notes there is nothing on the wall.
Nurse Melinda: I don’t see any spiders, but I understand that must be very scary for you. You're safe here with me.
Nurse Melinda conducts a brief cognitive screening and determines that Kadija is oriented to self, but not time, place, or situation.
Next, Nurse Melinda analyzes these cues. She reviews the electronic health record, or EHR, and notes that Kadija has no history of psychiatric illness.
Nurse Melinda recognizes that underlying factors, such as infection, fever, pain, sleep deprivation, fluid and electrolyte imbalance, as well as certain medications, can lead to alterations in a patient’s mental status, causing problems like delirium, especially in patients with advanced age and preexisting medical conditions.
She also recalls that delirium can develop over several hours or days and can result in a waxing and waning of mental function, including memory, thinking, language, behavior, mood, and personality. Hallucinations and delusions also often occur.
Nurse Melinda realizes that Kadija needs management of her altered mental status.
Sources
- "Varcarolis’s Canadian psychiatric mental health nursing. (3rd ed.)" Elsevier (2023)
- "Keltner’s psychiatric nursing. (9th ed.). " Elsevier (2023)