Coagulation studies - Partial thromboplastin time (PTT): Nursing
Coagulation studies - Partial thromboplastin time (PTT): Nursing
Watch later
Watch later
Notes
| COAGULATION STUDIES - PARTIAL THROMBOPLASTIN TIME (PTT) | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
A 2-year-old male is brought to the clinic by his mother because of a bloody nose that has continued to bleed for over an hour. The mother reports that her son has a history of easy bruising and is worried because one of her relatives has “some type of clotting disorder.” The child is holding a bloody cloth to his nose, with blood visible under his nose, mouth, chin, and T-shirt. On assessment, bright red blood is dripping from his nose. Based on these findings, the health care provider is concerned about a clotting disorder and orders a series of coagulation studies, including partial thromboplastin time.
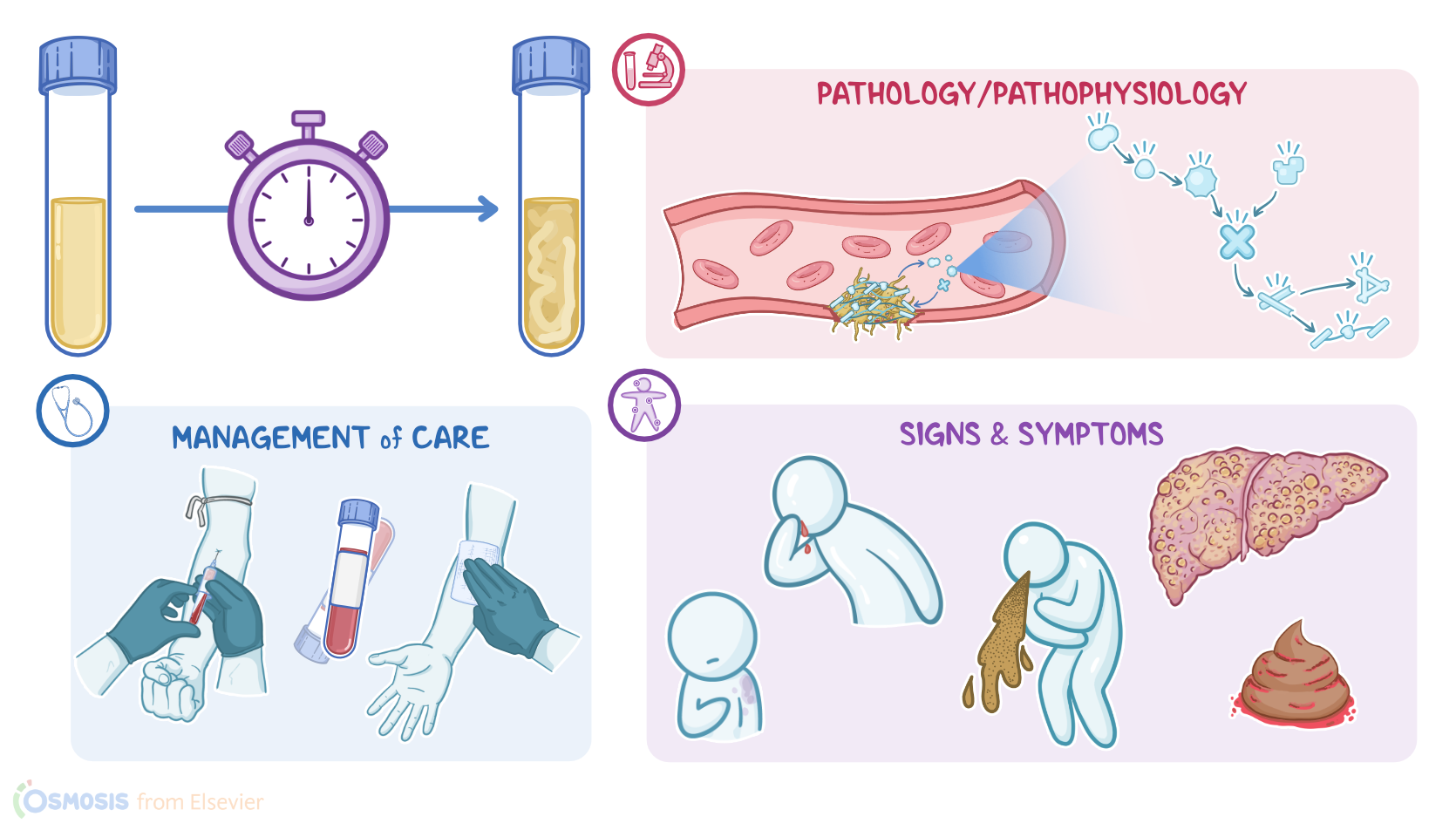
Now, normally, bleeding is stopped by the process of hemostasis. First, platelets stick together to form a plug. Then, the coagulation cascade is activated, which involves several clotting factors that interact within the intrinsic, extrinsic, and common pathways, ultimately creating a mesh that stabilizes the clot to help stop bleeding.
Now, partial thromboplastin time, or PTT for short, assesses the intrinsic pathway by measuring, in seconds, the time it takes to form a clot. An activated partial thromboplastin time, or aPTT, is when an activator is added to the sample to speed up clotting time and produce a more narrow range. So, the normal range for PTT is 60 to 70 seconds, while the normal range for aPTT is 25 to 30 seconds, depending on the activator used. The critical level for PTT is 100 seconds and 70 seconds for aPTT.
Alright, PTT can be increased if there aren’t enough clotting factors, which can happen due to reduced production, inactivation, or if the clotting factors get used up.
First up, inherited clotting disorders can cause a deficiency of a single factor, like with hemophilia A, when factor VIII is missing; and in hemophilia B, when factor IX is missing. Likewise, in von Willebrand disease, there’s no von Willebrand factor, which is a plasma protein that helps platelets stick to injured blood vessels, and acts as a carrier for clotting factor VIII.
Next, since clotting factors are created by the liver, severe liver disease like cirrhosis can reduce clotting factor synthesis.
Another way PTT can increase is if a clotting factor is inactivated. This can happen therapeutically when clients are given heparin, a medication that inactivates factor II, to prevent clotting. Finally, clotting factors can be depleted in disseminated intravascular coagulation, or DIC, which causes widespread thrombosis that uses up clotting factors.
Alright, PTT is typically measured if there are signs or symptoms of impaired coagulation like easy bruising; hematoma formation, which is a collection of blood in the tissues; hemarthrosis or bleeding in the joints; excessive epistaxis, also known as nosebleeds; or gastrointestinal bleeding, which could present as either blood in the stool or emesis.