Coagulation studies - Prothrombin time (PT) and international normalized ratio (INR): Nursing
Notes
| COAGULATION STUDIES - PROTHROMBIN TIME (PT) AND INTERNATIONAL NORMALIZED RATIO (INR) | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
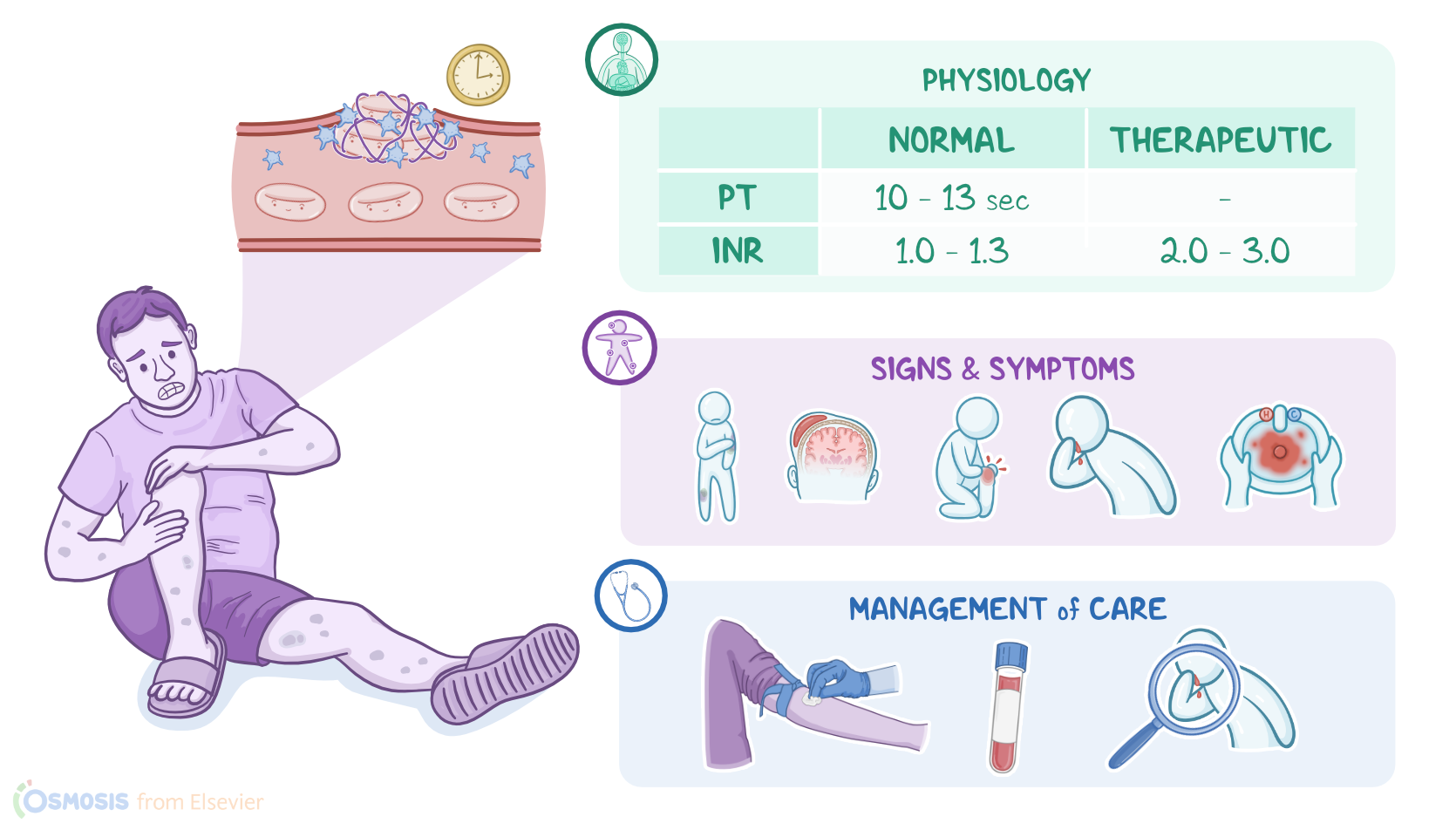
A 48-year-old male is brought to the emergency department by his wife because of severe knee pain after falling while cleaning the garage. His medical history is positive for a mechanical mitral valve replacement with subsequent anticoagulation using warfarin. On assessment, the client’s knee is swollen and tender to palpation; he appears pale and there are multiple bruises on his arms and legs. Based on these findings, the health care provider suspects overcoagulation and orders a prothrombin time and international normalized ratio.
Now, normally, bleeding is stopped by the process of hemostasis. First, platelets stick together to form a plug. Then, the coagulation cascade is activated, which involves several clotting factors that interact within the intrinsic, extrinsic, and common pathways, ultimately creating a mesh that stabilizes the clot to help stop bleeding.
Alright, prothrombin time, also known as pro time or just PT, measures the time, in seconds, it takes to form a clot. It is used to evaluate the extrinsic pathway.
Similarly, the international normalized ratio, or INR for short, is the time it takes to form a clot presented as a ratio of the client’s PT to a control, or standardized, PT.
The normal values for PT range from 10 to 14 seconds, while INR ranges from 1.0 to 1.3. Now, there is a therapeutic value for INR, which is higher, for people that require some level of anticoagulation, like in the case of a mechanical heart valve. In this case, the INR range is 2.0 to 3.0. Typically, PT and INR are drawn together and referred to as PT/INR.
Alright, the PT and INR can be increased if there aren’t enough clotting factors, which can happen due to reduced production, or if the clotting factors get used up.
Now, since clotting factors are created by the liver, severe liver disease like cirrhosis can reduce clotting factor synthesis. Now, the liver needs a supply of vitamin K to make clotting factors II, VII, IX, and X. So, another way PT and INR can increase is when clients are given a vitamin K antagonist, like warfarin, to therapeutically prevent clots from forming, like in clients with mechanical heart valves or atrial fibrillation.
Finally, clotting factors can be depleted in disseminated intravascular coagulation, or DIC, which causes widespread thrombosis that uses up clotting factors.
Alright, a PT/INR is typically measured if there are signs or symptoms of impaired coagulation like easy bruising; hematoma formation, which is a collection of blood in the tissues; hemarthrosis, or bleeding in the joints; excessive epistaxis, also known as nosebleeds; or gastrointestinal bleeding, which could present as either blood in the stool or emesis.
PT/INR is also measured to monitor liver disease, to establish the client's baseline PT/INR before starting anticoagulation therapy, and to monitor the effectiveness of warfarin therapy.