Components of the birth process: Nursing
Notes
| COMPONENTS OF THE BIRTH PROCESS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| POWER |
| |
| PASSAGE |
| |
| PASSENGER |
| |
| PSYCHE |
| |
Transcript
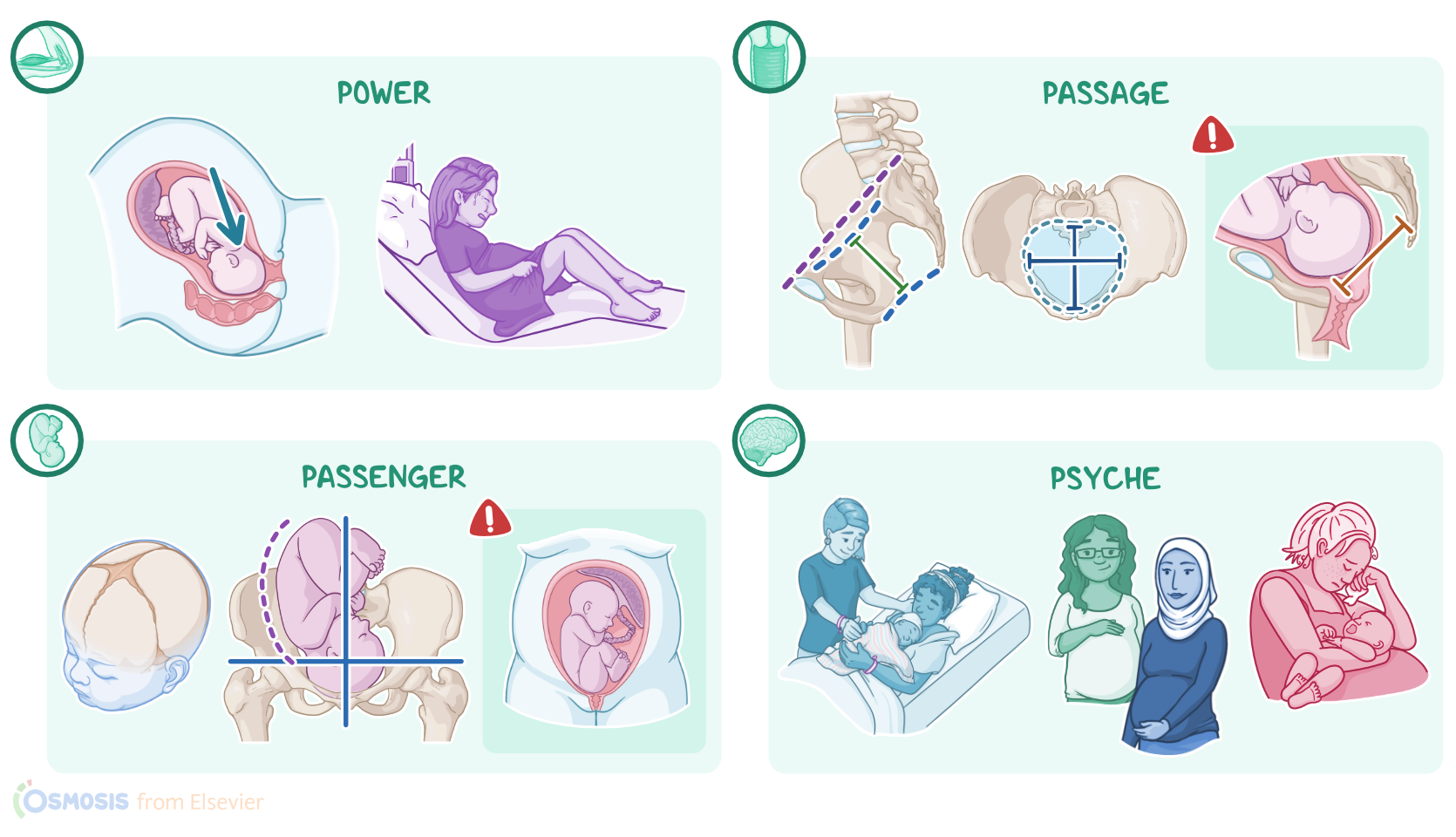
The main components of the birth process refer to the factors that interact with each other during childbirth. These components are grouped into 4Ps: power, which refers to uterine contractions and maternal pushing efforts; passage, which refers to the maternal pelvis that the baby passes through during labor; passenger, which refers to the fetus and placenta; and psyche, which refers to the client’s psychological status during labor.
Now, let’s look at each of these components, starting with power. Involuntary uterine contractions are the primary force of labor that dilate and efface the uterine cervix, after which maternal pushing efforts kick in. The descending fetus puts pressure on the vaginal wall and the rectum, which triggers the urge to push. These pushing efforts aid uterine contractions to push the fetus through the maternal pelvis.
The next P stands for passage, namely the maternal soft tissues, like the cervix, as well as the pelvis. Now, during labor, the cervix dilates and effaces, meaning it gets wider and thinner, to allow for an easier passage of the fetal head.
The pelvis is divided by an imaginary line called the pelvic brim into the upper or false pelvis, and the lower or true pelvis. The true pelvis is divided into the pelvic inlet above; the pelvic cavity in the middle; and the pelvic outlet below. Now, the right and left sides of the maternal pelvis are connected by cartilage called the symphysis pubis. During pregnancy, a hormone called relaxin increases, which softens joints, including, the symphysis pubis, which helps it to widen somewhat during childbirth to help accommodate the fetal head.
Overall, the shape of the pelvis can be classified into 4 types: the wider, more open gynecoid pelvis; the narrower android pelvis; the narrow and elongated anthropoid pelvis; and the wide but shallow platypelloid pelvis. The pelvic shape, as well as the diameters of the pelvic inlet and outlet, can influence how easily the fetus can pass through. Depending on the relationship between the pelvis and the fetal head, a complication of labor called cephalopelvic disproportion can occur. This can be either because the fetal head is too large, or because the pelvic opening is too small, but either way, it makes passage significantly more difficult.
Okay, let’s switch to our next P, which stands for passenger, and refers to the fetus, the fetal membranes, and the placenta. Now, for the fetus, there are a few components that can influence childbirth, including the fetal head, fetal lie, fetal attitude, as well as fetal presentation and position.
Let’s start with the fetal head, which is composed of skull bones connected by sutures with intervening spaces, called fontanelles. The skull bones that engage with childbirth include the frontal, parietal, and occipital bones. Typically, the sutures and fontanelles allow these bones to move slightly and change shape to adapt to the shape of the maternal pelvis, a process called moulding. Fetal head diameters can also be measured to predict the course of labor, such as the occipitofrontal diameter, which measures the back of the fetal skull and around the front.
The next fetal component is the fetal lie, which describes the orientation of the fetal long axis to the maternal long axis. Typically, the fetal lie is longitudinal, meaning that the fetal long axis is parallel to the maternal long axis. Fetal lie can also be horizontal, which is when the fetal long axis is perpendicular to the maternal long axis.