Congenital heart defects - Acyanotic: Nursing
Notes
| CONGENITAL HEART DEFECTS - ACYANOTIC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
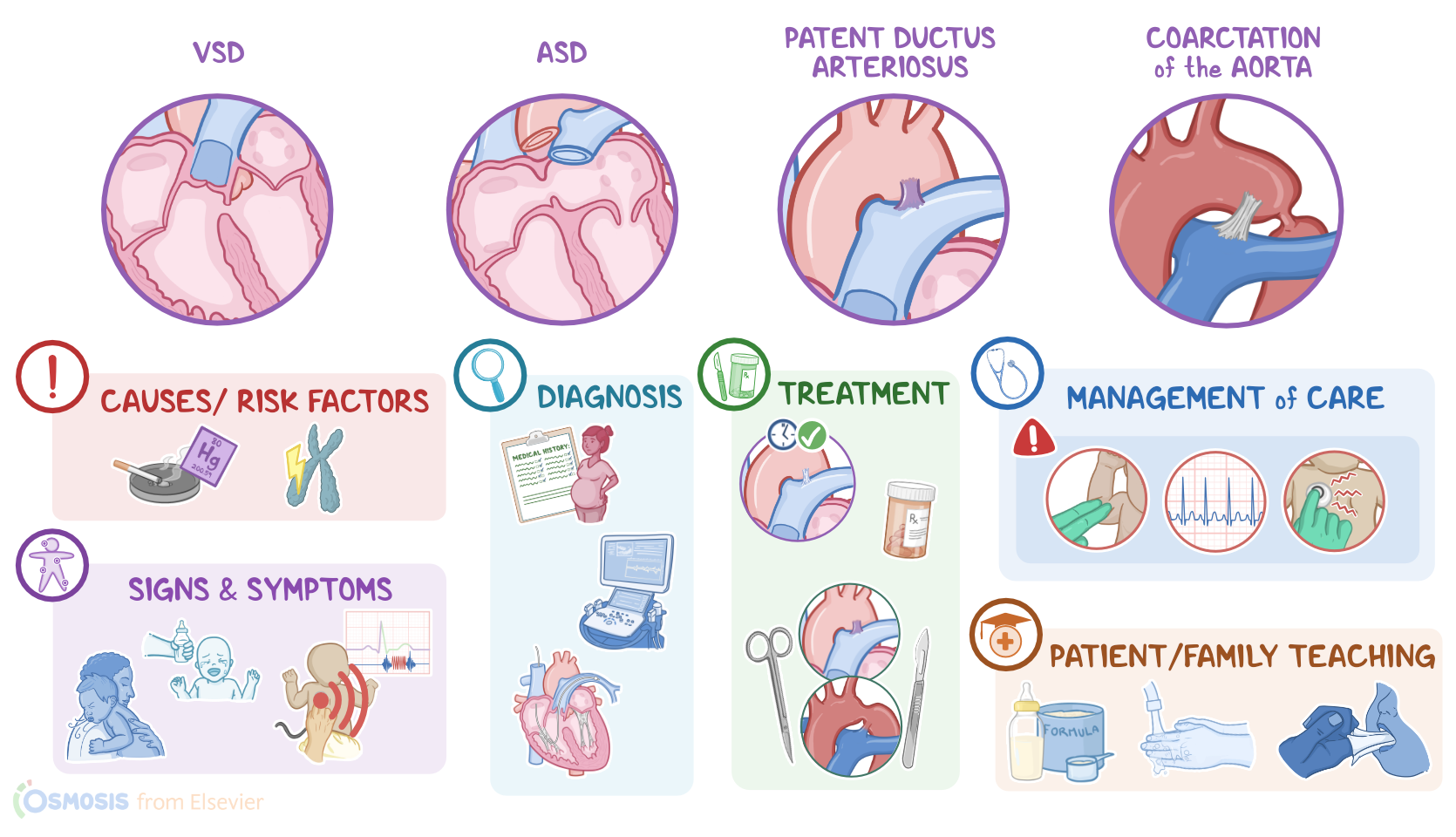
Congenital heart defects are cardiac conditions and anomalies that are present at birth. These are usually divided into two categories; aycanotic or cyanotic, based on the presence or absence of cyanosis, which means bluish discoloration of the skin. Congenital heart defects that don’t cause cyanosis are known as acyanotic heart defects. The main types of acyanotic heart defects are ventricular septal defect, or VSD for short, which is the most common one, in addition to atrial septal defect, or ASD, patent ductus arteriosus, or PDA, and coarctation of the aorta.
Now, let’s quickly recap the anatomy and physiology of fetal circulation. During fetal life, the lungs are filled with fluid and have high vascular resistance, so they don’t participate in gas exchange. Instead, the placenta serves as the organ of gas exchange, as well as delivering nutrients and removing metabolic wastes from the fetus.
So, oxygenated blood flows from the uterine arteries into the placenta, where oxygen passes through the capillaries and into the umbilical vein.
Then, part of the blood reaches the fetal liver, whereas about half of it bypasses the liver by a shunt called the ductus venosus, which diverts the oxygenated blood into the inferior vena cava, which has deoxygenated blood from the lower body.
Then, this blood flows into the right atrium and further mixes with deoxygenated fetal blood coming from the brain and upper body through the superior vena cava. Most of this mixed blood then moves through a small flap called the foramen ovale directly into the left atrium, into the left ventricle, and through the ascending aorta into the systemic circulation, supplying oxygen to the brain and upper body, as well as the lower body.
The rest of the blood from the right atrium flows into the right ventricle, and into the pulmonary arteries. A small amount of this blood moves into the pulmonary circulation and perfuses the lung tissue, but most of it is shunted through the ductus arteriosus back into the aorta and systemic circulation.
Ultimately, the blood flows from the systemic circulation into the umbilical arteries, and then back to the placenta.
At birth, when the umbilical cord is cut, the baby stops receiving oxygenated blood from the placenta. As a result, the baby’s blood has a reduction in oxygen levels, and an increase in its carbon dioxide levels. This change stimulates the respiratory center in the baby’s brain, which stimulates the newborn to take their first breath, along with temperature changes and tactile stimulation in the extrauterine environment.
This prompts a series of changes, which include lung expansion, and decreased pulmonary vascular resistance, allowing increased blood flow to the lungs.
In addition, there’s a functional closure of the foramen ovale and ductus arteriosus.
With time, the ductus venosus and umbilical vein, ductus arteriosus, and the umbilical arteries, atrophy then convert into ligaments.
Now, the exact cause of congenital heart defects is unknown, but it's believed to be associated with risk factors that can interfere with the development of the heart.
Common risk factors for all heart defects include chromosomal abnormalities of the fetus, in addition to maternal infections, chronic illnesses, and exposure to teratogens. The list of teratogens is long, and it includes things like medications such as isotretinoin, alcohol, recreational drugs like cocaine, tobacco smoke, and heavy metals like mercury.
Additionally, some specific risk factors for patent ductus arteriosus include premature birth, asphyxia during delivery, and rubella infection during pregnancy.
Now, the pathology of acyanotic congenital heart defects starts when a cardiac structure fails to form or close properly. The main types of acyanotic heart defects are ventricular septal defect, or VSD, atrial septal defect, or ASD, patent ductus arteriosus, or PDA, and coarctation of the aorta.
So, in the ventricular septal defect, there’s a gap in the ventricular septum, which separates the right and left ventricles. Likewise, in atrial septal defect, the gap is in the atrial septum, which separates the right and left atria. Next is patent ductus arteriosus, and that’s when the ductus arteriosus fails to close after birth. And finally, coarctation is a narrowing of the aorta which mostly occurs below the origin of the left subclavian artery at the origin of the ductus arteriosus.
Regardless of the type of defect, there’s a pathological communication between the left- and right-sided circulation. Due to the high pressure of the left side of the heart, the blood goes from the left to the right side of the heart and as a result, into the pulmonary circulation, and that is called left-to-right shunting. Because this extra blood is already oxygenated, there's no issue of cyanosis, but it does increase the pulmonary flow and that leads to pulmonary hypertension, which may progress into heart failure.
In some cases, over a long period of time, pulmonary hypertension becomes so severe that the pulmonary pressure exceeds the systemic pressure causing a reversal of blood flow from the right to the left side of the heart, called right-to-left shunting. This reversal is called Eisenmenger syndrome, and at that point, the deoxygenated right-sided pulmonary blood gets shunted to the left-sided systemic circulation, causing cyanosis.
Finally, some other complications of acyanotic heart defects include arrhythmias, embolism, and infective endocarditis.
Ok, now, clients with acyanotic heart defects are typically asymptomatic, but some clients can develop tachypnea, tachycardia, and activity intolerance. Some clients can also experience feeding problems, which can cause poor weight gain, and failure or difficulty to thrive.
On auscultation of the heart,defects can cause murmurs. These murmurs depend on the type of defect. For example, a ventricular septal defect typically causes a pansystolic murmur, and interestingly, it’s louder and harsher in small defects, and softer in larger ones. Atrial septal defects, on the other hand, can be heard as a soft, midsystolic murmur often described as a swishing sound. With PDA, there could be a continuous systolic murmur that extends into diastole. Finally, coarctation of the aorta could also cause a systolic murmur, but the most characteristic finding is a difference between upper and lower limb blood pressure, with blood pressure in the upper limbs being higher; and pulses in the lower extremities will be decreased or absent.
The diagnosis of acyanotic heart defects starts with the mother’s history during pregnancy and physical assessment of the client, followed by echocardiography to visualize the defect.
Most defects can also be detected prenatally by standard obstetric ultrasound examination. Additional imaging tests, such as a chest x-ray, CT, and MRI, might also be performed. An ECG is also required to look for arrhythmias.