Craniosynostosis: Nursing
Notes
| CRANIOSYNOSTOSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Craniosynostosis is a congenital disorder characterized by the premature closure of a cranial sutures that may lead to deformity of the skull shape and inhibition of brain growth.
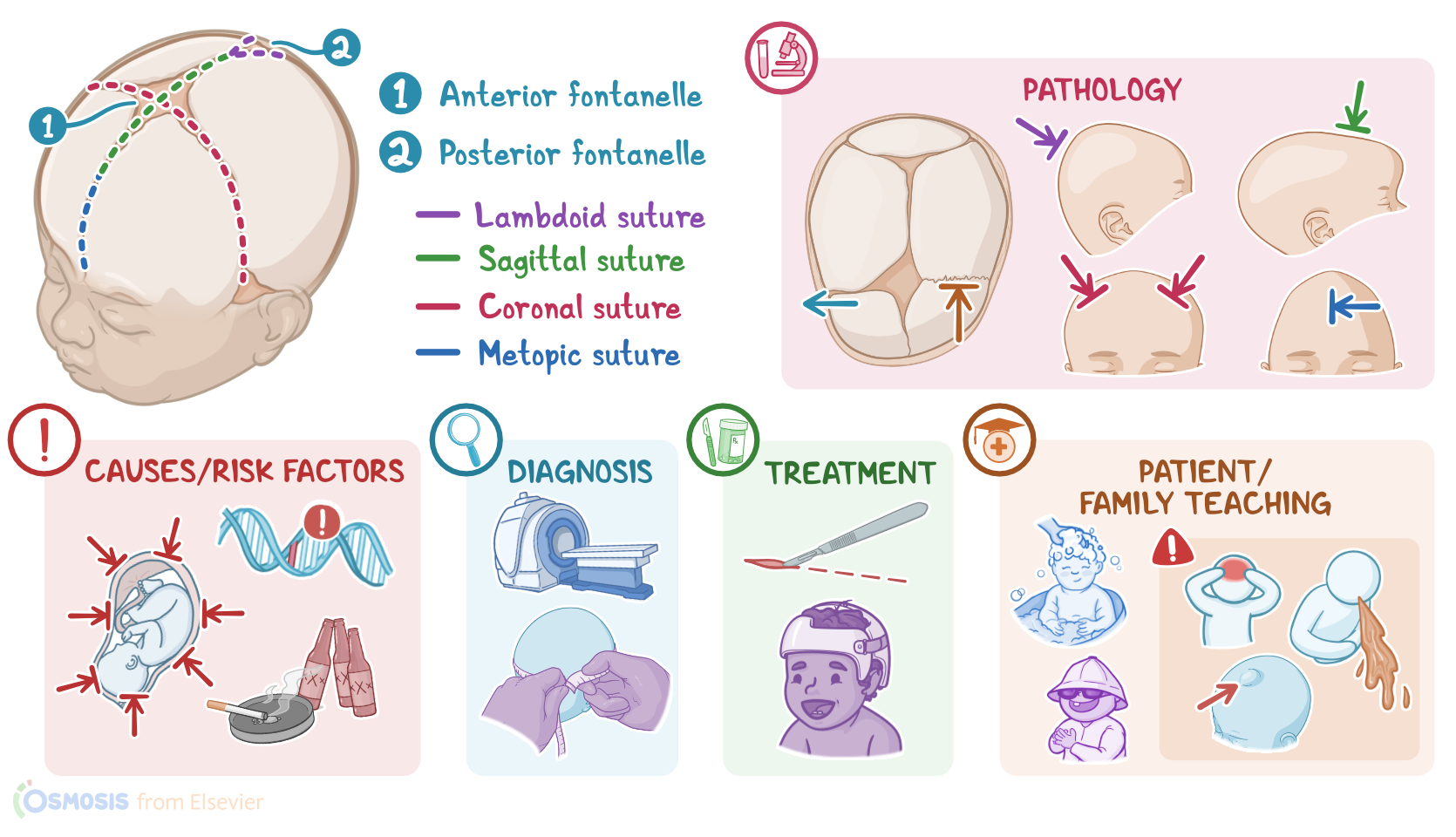
Now, the skull consists of the paired frontal bones, the paired parietal bones, and the isolated occipital bone. The spaces between the skull bones are called cranial sutures and there are four major sutures: metopic, coronal, sagittal, and lambdoid. The sagittal, coronal, and metopic sutures meet at the anterior of the skull to form the anterior fontanelle, palpable just behind the forehead at the midline. The posterior fontanelle is formed by the intersection of the sagittal and lambdoid sutures.
At birth, the cranial bones and sutures are not well developed and are not fused to accommodate momentary skull distortion at birth and allow brain growth and development after birth. At two months of age, the posterior fontanelle closes, followed by the closure of the anterior fontanelle at around 2 years old. The metopic cranial suture also closes at two years of age and all other sutures close in adulthood upon completion of the craniofacial growth.
Alright, now the exact causes of craniosynostosis are unknown, but it can be classified as non-syndromic, or isolated, which is the most common type, and syndromic, which is associated with other anomalies of the face, trunk, or extremities.
Risk factors for craniosynostosis include, maternal use of tobacco, alcohol, or other substances during pregnancy, advanced maternal age, and family history of craniosynostosis. Other causes include intrauterine constraint, where there’s pressure on the fetal skull during gestation, which can happen with maternal uterine malformations, multiple birth, or oligohydramnios, where there is not enough amniotic fluid to expand the uterine cavity.
Okay, moving on to pathology, craniosynostosis occurs when there’s a premature fusion of one or more cranial sutures, which restricts the growth of the skull perpendicular to the affected suture. To accommodate the growth of the brain, the skull will grow parallel to the affected suture. The resulting skull deformity depends on the type of suture that is affected. So, according to the affected suture, craniosynostosis can be classified into 5 types, including sagittal, metopic, unilateral coronal, bicoronal and lambdoid craniosynostosis.
Starting with sagittal craniosynostosis, also known as scaphocephaly, this is the most common form, and results from the premature fusion of the sagittal suture. It’s characterized by a long and narrow growth of the head in the anteroposterior direction, and also a broad forehead and a prominent occiput.
Metopic craniosynostosis, also known as trigonocephaly, results from the premature fusion of the metopic suture, and is characterized by a triangular shaped forehead. The eyebrows may appear pinched on either side, and the eyes may also appear close together. Down the forehead, a ridge can usually be felt.
Next, unilateral coronal craniosynostosis is known as anterior plagiocephaly, while lambdoid craniosynostosis is known as posterior plagiocephaly. So, anterior plagiocephaly is caused by the early fusion of one side of the coronal suture, and is characterized by a flattened forehead and orbital rim on the affected side and a different shape of the eye on the affected side. On the other hand, the posterior plagiocephaly is caused by the early fusion of the lambdoid suture and is characterized by a flattening of the back of the head.
Finally, bicoronal craniosynostosis, also known as brachycephaly, is caused by the early fusion of the coronal suture bilaterally. It’s characterized by a wide shaped head with a very flat and tall forehead and the skull shortened in the anteroposterior direction.
Important complications associated with craniosynostosis include prolonged restriction of the cranial growth, which can result in increased intracranial pressure, or ICP, hydrocephalus, and inhibition of the brain growth. Inhibition of brain growth can lead to impairment of the cognitive and neurodevelopment functions, and if the cranial nerves are involved, deficits in vision, hearing, and speech might occur.
In the terms of clinical manifestations, the first sign of craniosynostosis is an abnormally shaped skull which can vary depending on the affected suture. Other signs may include an absence of soft spot on the baby’s skull, called a fontanelle; a raised firm edge where the sutures close; and delayed or absence of growth in the baby’s head size over time.