Encephalitis: Nursing
Encephalitis: Nursing
Medical Surgical
Medical Surgical
Notes
| ENCEPHALITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Encephalitis is the inflammation of the brain, also known as the cerebrum, which can also involve the meninges, cerebellum, and brainstem.
Let’s start by looking at the physiology of the nervous system, which is divided into the central and peripheral nervous system. The central nervous system includes the brain and spinal cord, while the peripheral nervous system includes all the nerves that connect the central nervous system to the muscles and organs. The brain is divided into the cerebrum, which consists of the two cerebral hemispheres, the cerebellum, which sits down at the base of the skull, and the brainstem, which is located right in front of the cerebellum.
Now, the brain is protected from the rest of the body by three meningeal layers. From outside to inside, these are the dura mater, arachnoid mater, and pia mater. Between the arachnoid and pia mater there’s the subarachnoid space, which houses the cerebrospinal fluid. The cerebrospinal fluid is a clear, watery liquid that cushions the brain from impact and bathes it in nutrients.
Zooming in, the cells that make up our brain are called neurons and they receive and send electrical impulses to one another. Now, neurons need a lot of oxygen and nutrients to function properly, so the brain has a rich blood supply. But for any nutrients to enter and leave the brain, they have to go through the tightly regulated blood-brain barrier. This refers to the endothelial cells in the blood vessels of the brain which are so tightly bound to one another that they only allow certain molecules to slip through them.
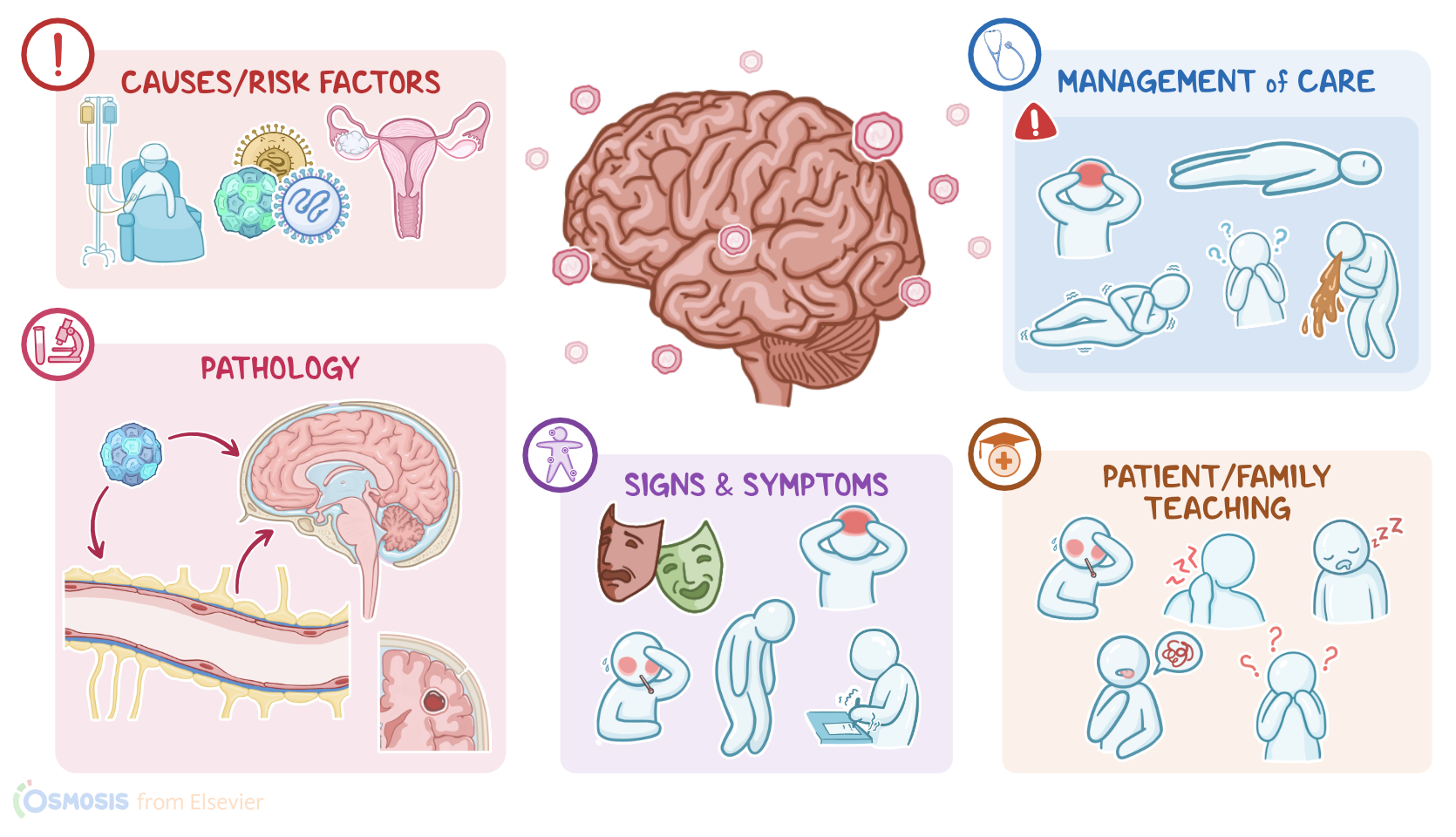
Now, in most cases, encephalitis is caused by a virus, such as herpes simplex virus, or HSV for short; enteroviruses, like echovirus and coxsackie virus; West Nile virus; rabies; mumps; and measles. Varicella zoster virus and cytomegalovirus can also cause encephalitis, particularly in immunocompromised clients. Less commonly, encephalitis can be caused by bacteria, fungi, or parasites. Very rarely, encephalitis can be autoimmune in nature, in which case it can occur as a consequence of cancer somewhere else in the body, like the ovaries.
Risk factors for encephalitis include clients under 1 or over 55 years of age, or clients who are immunosuppressed, such as those who have HIV. Encephalitis is also more common during the summer months and in places rich with mosquitoes or ticks. Alright, now, regardless of the cause, there are three routes that an infection can take to reach the brain. The first way is direct spread, which is when a pathogen gets inside the skull, for example through a skull fracture, and then penetrates the meninges, eventually ending up in the brain. The second way is hematogenous spread, which is when a pathogen enters the bloodstream and moves through the endothelial cells in the blood vessels making up the blood-brain barrier and gets into the brain. Finally, certain pathogens, such as the rabies virus, can move in a retrograde fashion from the peripheral nervous system to the brain. Once inside the brain, the pathogen starts multiplying. In response to this, the immune system launches an inflammatory response, which results in brain edema, increasing the pressure inside the skull. This can in turn reduce blood flow to the brain, which may cause neuronal activities to slow down and affect various brain functions, such as the control of movement, mood, or behavior.
In severe cases, encephalitis may cause acute complications, such as the formation of a brain abscess, where pathogens wall off from the rest of the brain parenchyma. Another complication is intracerebral hemorrhage or bleeding inside the brain. Although rare, encephalitis can also cause long-term complications, such as extensive brain damage.
Clients with encephalitis typically present with fever, fatigue, and headache. Additionally, there can be signs of increased intracranial pressure such as vomiting, as well as the Cushing triad, which includes bradycardia, irregular respiratory pattern, and hypertension. Signs of meningeal irritation can also be present, including nuchal rigidity, in addition to Brudzinski and Kernig signs. In Brudzinski sign, flexion of the neck causes hip and knee flexion, whereas in Kernig sign, flexion of the hip and knee to 90 degrees causes pain in the neck.