Epistaxis: Nursing process (ADPIE)
Epistaxis: Nursing process (ADPIE)
FINAL
FINAL
Notes
| EPISTAXIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
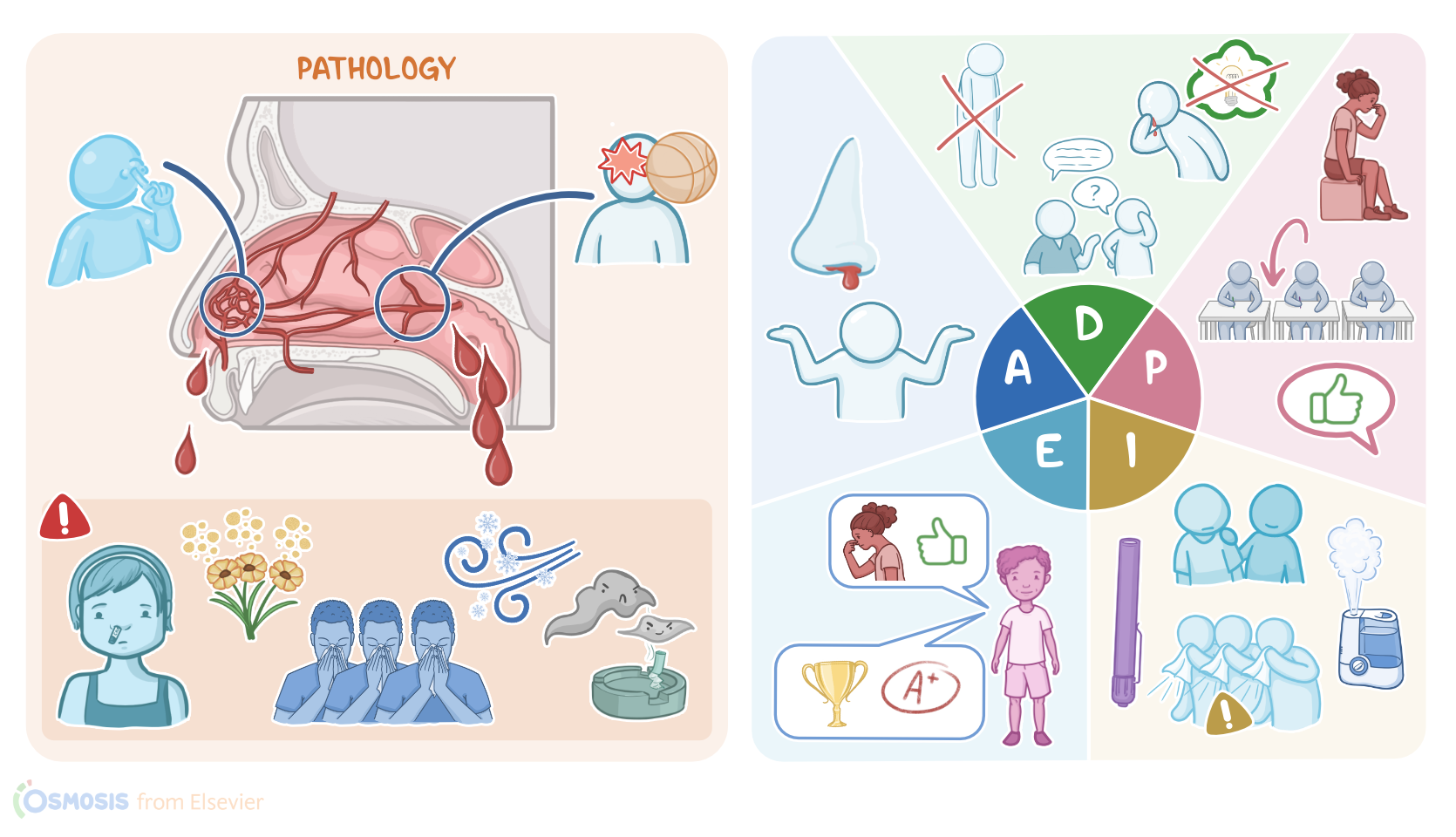
Ethan Porter is a 10-year-old student who was brought to the school nursing office by his gym teacher with a nosebleed.
Ethan was newly diagnosed with von Willebrand disease, and about 5 minutes ago, his nose suddenly started bleeding while he was running the track outside in gym class.
Epistaxis, or nose bleed, is caused by ruptured blood vessels in the nasal mucosa.
Up to 90% of epistaxis is anterior epistaxis where bleeding occurs in the anterior nasal cavity and the blood typically comes out of the nares.
Posterior epistaxis occurs in the superior or posterior nasal cavity so the blood usually goes down the throat.
In the anterior nasal cavity, numerous arteries in the face connect together to form the Kiesselbach’s plexus, also known as Little's area.
This blood vessel rich area is located on the nasal septum and is covered by a thin mucus membrane that offers little protection so dryness, irritation or even minor trauma, like nose picking, can lead to bleeding.
An intranasal mass and foreign bodies can also be causes.
The most common sign is visible bleeding, usually from one nostril.
After having the person gently blow their nose to clear blood clots, the nasal cavity is typically assessed with a light source and a nasal speculum to look for signs of active bleeding, excoriation, or scabbing.
Posterior epistaxis occurs further back in the nose, and the most common site is where blood vessels come together in the lateral wall of the nasal cavity to form the Woodruff’s plexus.
Since it’s located deeper in the nasal cavity, more severe head and nasal trauma can cause this type of epistaxis.
It is more serious than anterior epistaxis because the bleeding is often more severe and blood can go down the pharynx, esophagus and trachea.
If blood goes down the trachea it can cause coughing and hemoptysis, while swallowing blood can cause nausea, vomiting and hematemesis.
If bleeding occurs frequently it could even lead to anemia.
Due to the posterior location of the bleeding, a client with posterior epistaxis could appear asymptomatic or with very subtle signs like frequent swallowing.
Sometimes the blood will come out the nostrils and resemble an anterior epistaxis.
Now, let’s look at the common risk factors for epistaxis. Children, especially those between the ages of 2 and 10 are at a higher risk.
Frequent nose picking, playing contact sports or the lack of proper protective equipment like a face guard can increase the risk of trauma.
Allergies, upper respiratory tract infections, tobacco smoke, cold or dry environments can cause chronic irritation.
Also frequent and forceful nose blowing could also cause damage to the blood vessels.
There are also systemic risk factors like coagulopathies. Common ones include hemophilia and von Willebrand disease.
People 45 to 65 have decreased platelet levels and they are more likely to be taking medications like aspirin and warfarin that can interfere with clotting.
Pregnant people can also be prone to epistaxis due to expansion of nasal blood vessels and increased venous pressure.
Diagnosis of epistaxis can often be made based on the visualization of blood from the nose, especially for anterior epistaxis.
However, the oral cavity should always be checked to see if there are signs of posterior epistaxis.
In cases of prolonged or recurrent bleeding, it’s important to identify the cause.
Visual inspection with the use of a nasal speculum can help identify the source of bleeding as well as potential causes such as a foreign objects.
An endoscope can be used to pinpoint the source of a posterior epistaxis.
Coagulopathies like hemophilia and von Willebrand disease should also be suspected when there’s prolonged or recurrent bleeding especially if they also have a history of prolonged bleeding from the mouth, gums, and IV sites, or easy bruising.
Epistaxis is frequently managed outside of the healthcare setting without complications.
The first step is to make sure the client’s airway is clear and they are hemodynamically stable.
Next, management of bleeding begins with having the person sit or stand upright and tilt their head forward.
This prevents blood from draining backwards.
Pressure is applied to the soft area just underneath the nasal bones with a thumb and forefinger.
The nares should be compressed firmly against both sides of the septum.
The person should be breathing through an open mouth, and continue holding pressure for 10 to 15 minutes.
A young child will likely need someone else holding pressure for them and helping them to remain calm.
If bleeding persists, keep holding pressure and apply ice packs to the nasal bridge, cheeks, upper lip, or back of the neck to aid in vasoconstriction.
If bleeding continues after 10 minutes of applying pressure, medical attention should be sought.
If bleeding does resolve, the person should avoid laying down, bending over, straining, and sneezing.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Winter peaks in web-based public inquiry into epistaxis" Eur Arch Otorhinolaryngol (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Nontraumatic Aneurysm-An Unusual Cause of Epistaxis" Ear Nose Throat J (2022)
- "Management of idiopathic epistaxis in adults: what's new?" Acta Otorhinolaryngol Ital (2019)
- "Epistaxis: Revisited" Indian J Otolaryngol Head Neck Surg (2020)
- "Epistaxis: the cause found beyond the nose" Autops Case Rep (2020)