Foreign body aspiration and upper airway obstruction: Nursing process (ADPIE)
Foreign body aspiration and upper airway obstruction: Nursing process (ADPIE)
NRS 428 WK 2 ADPIE
NRS 428 WK 2 ADPIE
Notes
| FOREIGN BODY ASPIRATION & UPPER AIRWAY OBSTRUCTION | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Ali Jafari is a 11-month-old male brought to the emergency department, or ED, by his parents, who state that Ali was playing on the floor when he started to cough and choke.
They rushed him to the ED when Ali’s coughing got worse and started to have trouble breathing.
Ali is being treated for upper airway obstruction due to foreign body aspiration.
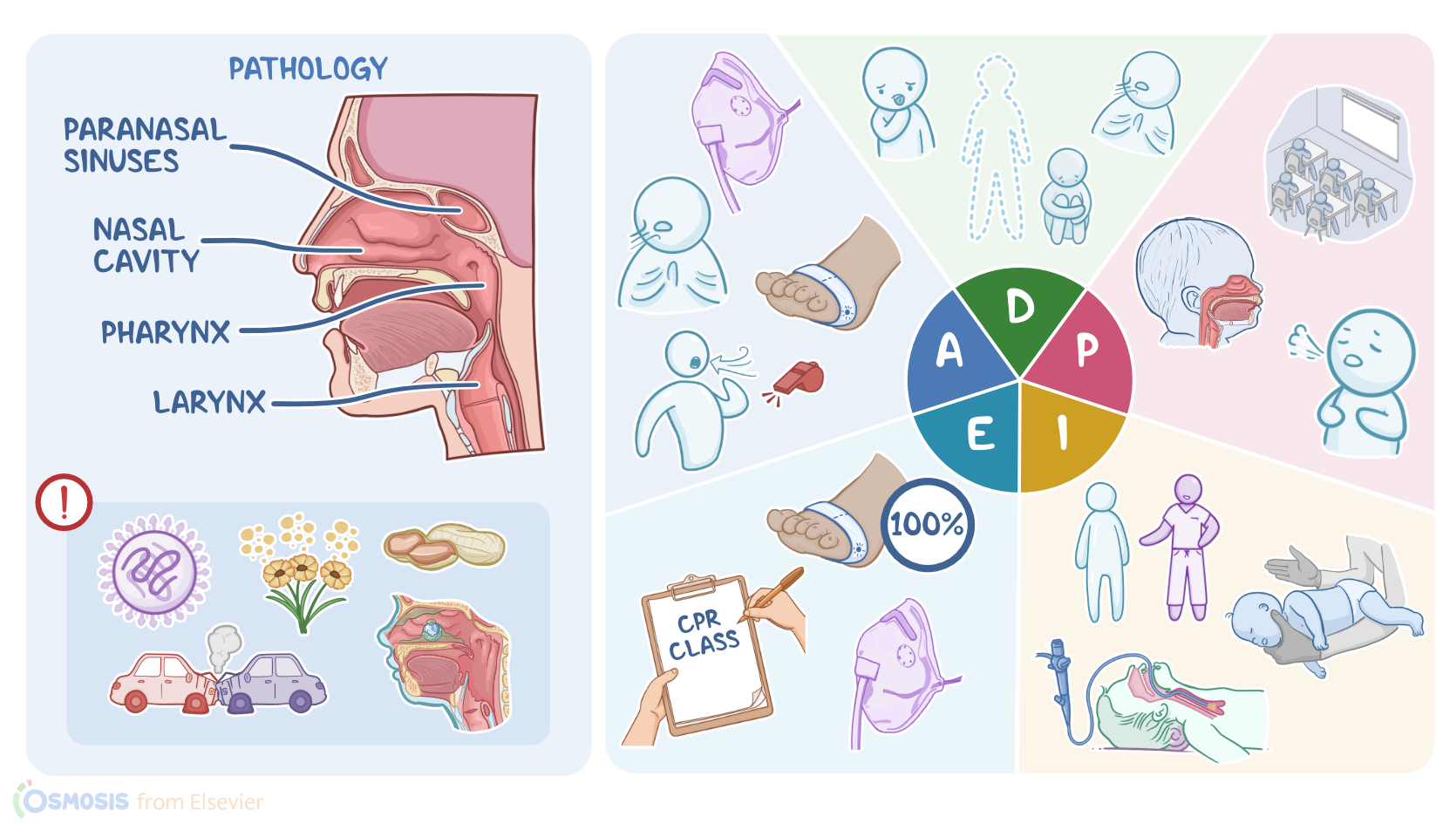
The upper airway consists of the nasal cavity, paranasal sinuses, pharynx, and larynx.
Any mass or edema in these regions can cause partial or complete obstruction.
One common cause is upper respiratory tract infections like croup, laryngitis, and epiglottitis which are typically caused by viruses, and can lead to inflammation which can cause edema and obstruction of parts of the upper airway.
Allergens like dust, pollen and pet dander can cause mild reactions like rhinitis and sinusitis where nasal discharge and congestion can lead to obstruction.
More severe reactions like anaphylaxis can occur when there’s severe allergic reactions to things like peanuts or shellfish.
This can lead to angioedema, which is a rapid and severe swelling of the mucosa, leading to obstruction.
Trauma that causes airway obstruction can include direct trauma like a car crash or gunshot wound which can collapse parts of the airway or cause bleeding that obstructs the airway.
Congenital anomalies include conditions like laryngomalacia which is an anomaly of the laryngeal tissues that causes a partially obstructed airway.
Finally, foreign body aspiration occurs when a foreign object, like a nut, coin, or small toy gets lodged in the airway.
It can happen to anyone, but occurs most commonly in young children who have a smaller airway diameter than adults.
They also like to explore by placing objects in their mouth and are easily distracted during eating which can increase risk of aspiration.
Children younger than 2 usually don’t have molars yet, so they are unable to grind their food into smaller more manageable pieces.
Small objects that are round and smooth like grapes, hot dogs, and balloons, are more likely to cause obstruction.
Batteries and magnets can cause additional damage as batteries may cause tissue corrosion, and magnets can trap tissue between them and cause necrosis of trapped tissue.
Most of the time, smaller foreign bodies will end up in the lower respiratory tract or lung because of gravity.
However, larger objects can get stuck in the upper airway and the symptoms can be more severe since air flow to both lungs become restricted.
With a partial airway obstruction, children may cough, gag, choke, drool, or experience dyspnea.
They may sound hoarse when they speak, and inspiratory stridor, a high pitch whistling sound, can be heard on auscultation.
When a complete obstruction occurs, children may be unable to cough, speak, or breathe and may become cyanotic or become unresponsive.
However, up to half of all children with a foreign body aspiration may be asymptomatic.
Initially, the child may cough and gag, but when the symptoms go away parents will often think nothing is wrong.
Persistent obstruction can lead to aspiration pneumonia, atelectasis, edema or abscess formation.
Diagnosis of foreign body aspiration is based on the child’s history and physical examination.
It’s important to ask what they were eating or playing with at the time, or what items might have been nearby.
Diagnostic imaging can be used but if there’s a risk of complete obstruction, oxygenation and securing the airway should be prioritized.
Imaging studies such as posterior-anterior and lateral neck X-ray can be done, but will only show items that are radiopaque, like coins and batteries.
Items like food and plastic are usually radiolucent and won’t appear, though overinflation, atelectasis, lung infiltrates may indirectly indicate the presence of a foreign object.
Fluoroscopy, which uses continuous X-ray imaging and contrast dye, or a CT scan can be done if X-ray is inconclusive.
False negatives can occur with imaging, so if there’s still suspicion of aspiration, endoscopy, specifically laryngoscopy, uses a small flexible scope to visualize the upper airway.
Treatment of upper airway obstruction depends on the cause and location of the obstruction. treatment is first focused on maintaining adequate ventilation, and oxygen is administered if needed.
In the case of severe or complete obstruction from foreign body aspiration in adults or children one year and older, the Heimlich maneuver should be attempted where five abdominal thrusts are done and repeated until the object is removed.
Children younger than one are placed face down across the forearm and five back blows are delivered followed by five chest thrusts.
If these maneuvers fail to remove the object, laryngoscopy is needed to visualize the object so it can be removed by forceps or suction.
If the child becomes unresponsive, cardiopulmonary resuscitation, or CPR should be performed.