Laryngeal cancer: Nursing
Laryngeal cancer: Nursing
Medical Surgical
Medical Surgical
Notes
| LARYNGEAL CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Laryngeal cancer is a malignant tumor that originates from the larynx, which is the part of the throat used for swallowing and talking.
First, let’s quickly review the anatomy and physiology of the larynx, which is located in the upper portion of the neck between the pharynx and the trachea. Now, the larynx can be divided into three main parts. The upper part, or the supraglottis, is located below the base of the tongue and includes the epiglottis, which closes off during swallowing, preventing food and liquids from entering the airway.
Next is the middle part, or glottis, which contains the vocal cords. When these are closed, air pressure builds up below them, causing them to vibrate and produce sound when we speak. Finally, the lower part, or subglottis, extends between the vocal cords and the start of the trachea.
Now, the larynx is lined with a stratified squamous epithelium which then transitions into a pseudostratified ciliated columnar epithelium. This contains goblet cells, which produce mucus to trap small foreign particles; as well as columnar cells, which have cilia, or tiny little hair-like projections that move mucus up the respiratory tract so it can be coughed out.
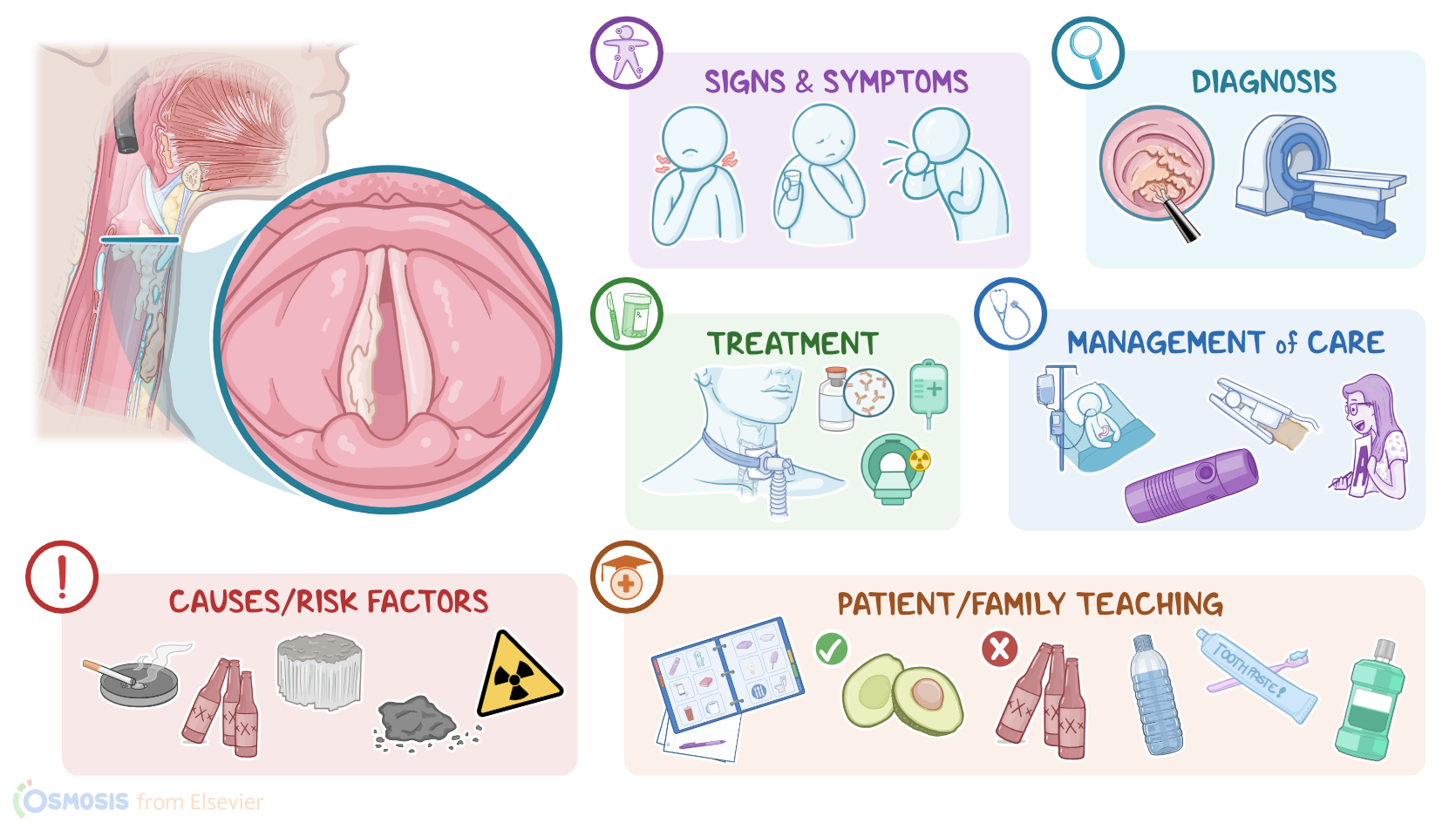
All right, now, laryngeal cancer occurs when any of these epithelial cells acquire mutations, which can arise due to a variety of risk factors. Modifiable risk factors include exposure to irritants, such as tobacco smoke, alcohol, asbestos, coal dust, and ionizing radiation. Other modifiable risk factors include obesity, infection with human papillomavirus, or HPV, as well as a history of gastrointestinal reflux disease, where acid from the stomach goes all the way up the esophagus into the pharynx. From there, the acid can contact and irritate the larynx. As for non-modifiable factors, few clients with a family history of laryngeal cancer are genetically predisposed to develop this type of cancer even without the presence of environmental risk factors.
So, chronic exposure to irritants can cause the normal columnar cells to undergo dysplasia, or abnormal growth. Depending on how much of the epithelium is affected by dysplasia, it can be divided into three grades. The higher the grade, the more likely the lesion will evolve into cancer. Eventually, if the irritation persists, dysplasia can evolve into carcinoma in situ, which affects the entire thickness of the epithelium. Finally, carcinoma in situ can progress to invasive laryngeal carcinoma, which is when cancerous cells break through the epithelial basement membrane into the underlying stroma, and may even spread to nearby lymph nodes or metastasize to distant organs, such as the lung, bones or liver.
All right, now the main signs and symptoms of laryngeal cancer include persistent voice hoarseness, sore throat, and dysphagia, because the mass may compress the esophagus, which can also lead to unintentional weight loss. Clients may also complain of pain or ringing in the ears, feeling a lump in the throat and hemoptysis. In late stages, the tumor can obstruct the airway, causing shortness of breath or impossible breathing altogether, which requires an emergency tracheostomy.
Now, the diagnosis of laryngeal cancer involves the client's history and physical assessment, followed by laryngoscopy to visualize the tumor. CT, or MRI scans of the larynx and the surrounding tissues can be used to stage the tumor in the TNM system, where T stands for tumor location and local spread; N stands for lymph node involvement; and M for whether or not the tumor has metastasized. Once a suspicious lesion is found on imaging, a biopsy is needed to confirm the diagnosis.
Treatment of laryngeal cancer depends on the size of the tumor and how much it has spread. There are various types of surgical interventions that can be done, including vocal cord resection, and partial or total laryngectomy. In addition to surgery, clients could be treated with chemotherapy, immunotherapy, or radiotherapy. Also, any involved nearby lymph nodes should be resected. Finally, if part or all of the larynx has been surgically removed, voice rehabilitation therapy or some devices, like an electrolarynx or a pneumatic larynx, can be used to facilitate communication.
All right, let’s look at the nursing care you’ll provide for a client with laryngeal cancer. Priority goals include maintaining a patent airway, ensuring adequate nutritional intake, providing postoperative care, and providing comfort and emotional support to promote quality of life.
First, assess your client’s vital signs and oxygen saturation, as well as their respiratory status. If your assessment reveals any indications of respiratory distress, such as dyspnea or a decreased oxygen saturation, report these findings to the healthcare provider. Assist them into a high Fowler position and administer supplemental oxygen. Then, assess their pain level including quality, location, severity, and timing, as well as relieving and provoking factors. Assist your client into a comfortable position, provide comfort measures, and administer analgesic medications as prescribed.
Next, perform a nutritional assessment by noting your client’s current weight, swallowing pattern, gag and cough reflexes. Ensure a referral to a speech pathologist and a registered dietician have been placed, and provide nutrition by administering the prescribed enteral feedings or oral nutrition, as tolerated. Immediately report to the healthcare provider if your client experiences coughing, signs of aspiration, shortness of breath, or chest discomfort.