Hemorrhagic stroke - Intracranial hemorrhage (ICH) and subarachnoid hemorrhage (SAH): Nursing
1,345views
Hemorrhagic stroke - Intracranial hemorrhage (ICH) and subarachnoid hemorrhage (SAH): Nursing
Neurological Disorders
Neurological Disorders
Notes
| HEMORRHAGIC STROKE - INTRACEREBRAL HEMORRHAGE (ICH) AND SUBARACHNOID HEMORRHAGE (SAH) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Contributors
Stroke, also known as cerebrovascular accident or brain attack, is when the brain gets damaged due to being deprived of oxygen-rich blood. There are two main types of stroke: ischemic stroke, which occurs when there’s a blockage of an artery, and hemorrhagic stroke, which occurs when an artery in the brain leaks into the brain tissue.
First, let’s discuss the anatomy and physiology of the brain, which has three main parts called the cerebrum, cerebellum, and brainstem. The cerebrum is the most obvious part of the brain and it’s divided into two cerebral hemispheres, each of which has four lobes, called the frontal, temporal, parietal, and occipital lobe. The frontal lobe controls eye and voluntary movement. There’s also a specific region of the frontal lobe called Broca’s area, which controls speech production. Next, there’s the temporal lobe, which plays an important role in long-term memory formation, and recognition of faces, scenes, and speech. The temporal lobe also has an area called Wernicke’s area, which is in charge of understanding spoken and written language. Both Broca’s and Wernicke’s areas are located in the dominant hemisphere, meaning the left hemisphere for right-handed people, and right hemisphere for left-handed people. Finally, the parietal lobe is responsible for sensory perception; while the occipital lobe plays an important role in visual processing.
Now, the cerebellum helps with muscle coordination and balance; while the brainstem refers to the part of the central nervous system that connects the brain with the spinal cord. Within the brainstem, descending motor fibers from the left and right cerebral hemispheres decussate, meaning they cross over to the opposite side, and eventually make their way down to the spinal cord. This makes it so that the right cerebral hemisphere controls muscles on the left side of the body and vice versa. The brain stem also contains the nerve cell bodies of cranial nerves, as well as cardiovascular and respiratory centers, which play a vital role in functions like heart rate, blood pressure, and breathing.
Now, both the brain and spinal cord are covered with protective membranes called meninges. The outer layer of the meninges is the dura mater, the middle layer is the arachnoid mater, and finally, the inner layer is the pia mater. Between the arachnoid mater and the pia mater is the subarachnoid space, which houses cerebrospinal fluid, or CSF for short, as well as the arteries that supply the brain. Cerebrospinal fluid is a clear, watery liquid that is pumped around the spinal cord and brain, bathing them in nutrients and cushioning them from impact. And finally, let’s look at cerebral circulation. The brain receives blood from the left and right internal carotid arteries, as well as the left and right vertebral arteries, which come together to form the basilar artery. The internal carotid arteries give rise to the left and right middle cerebral arteries, which serve the lateral portions of the frontal, parietal, and temporal lobes of the brain; and also to the anterior cerebral arteries, that nourish the medial portions of the frontal and parietal lobes.
On the other hand, the basilar artery gives off the right and left posterior cerebral arteries, which mainly serve the occipital lobe, some parts of the temporal lobe, and thalamus. Additionally, the vertebral arteries and the basilar artery also give branches for the cerebellum and brainstem.
Now, the anterior cerebral arteries connect with one another over a short connecting blood vessel called the anterior communicating artery, while the internal carotid and the posterior cerebral arteries connect through the posterior communicating artery, which is a branch of the internal carotid itself. Together, the anterior and posterior cerebral arteries, along with the internal carotids, the single anterior communicating artery and the two posterior communicating arteries form the Circle of Willis, which is a network of anastomoses that allow uninterrupted blood flow to the brain even when one of the vessels is obstructed.
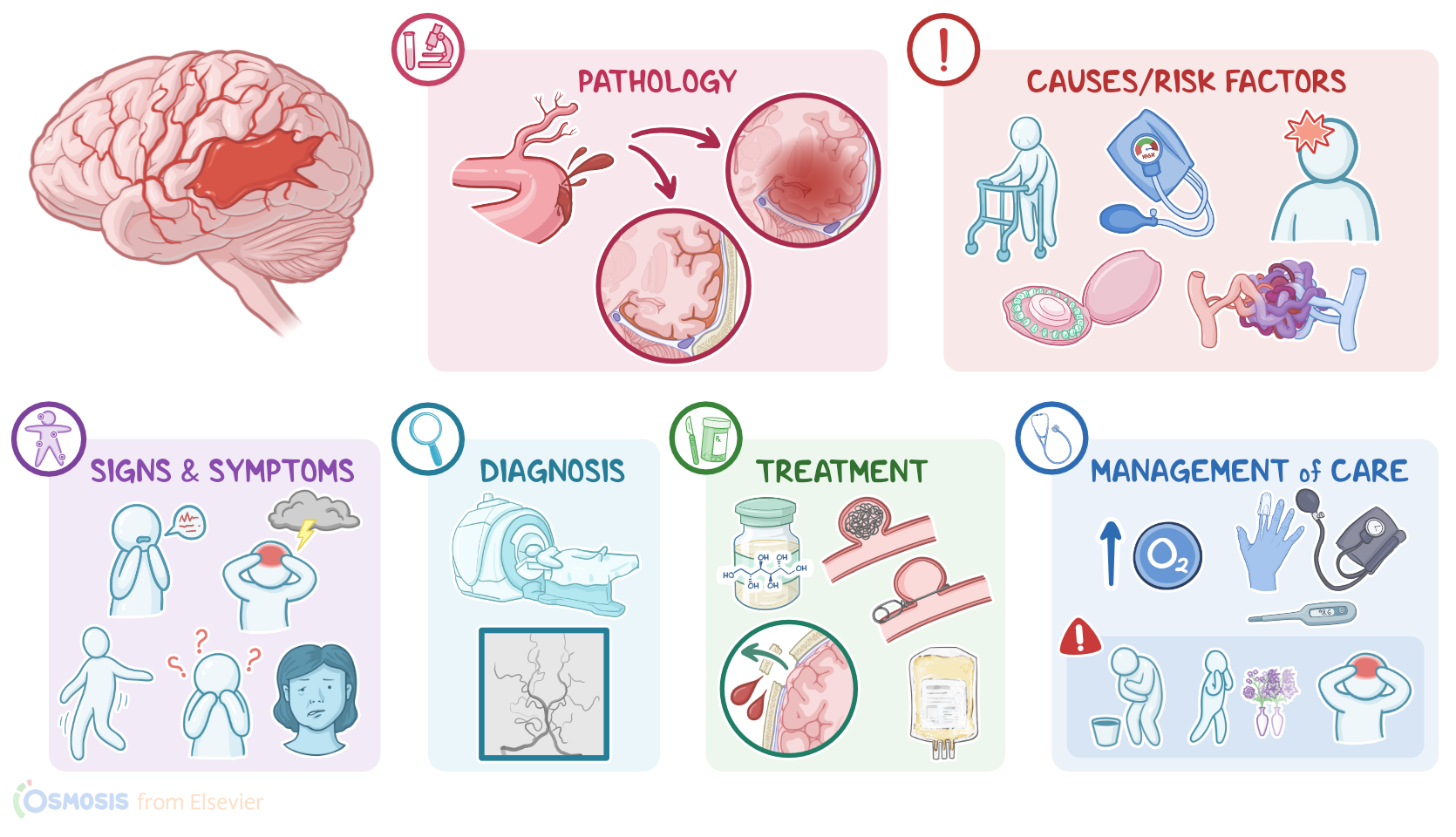
Now, the main cause of hemorrhagic stroke is the rupture of a cerebral blood vessel. Important factors that increase the risk of rupture can be divided into two main groups. The first group covers individual risk factors, such as age over 55, obesity, and the use of alcohol, tobacco, and cocaine. Other important individual factors include the use of oral contraceptives or the use of anticoagulant medications.
The second group covers conditions associated with hemorrhagic strokes, such as uncontrolled hypertension, which is the most important one, as well as the presence of cerebral aneurysms and arteriovenous malformations. Other conditions that put a client at risk for hemorrhagic stroke include previous strokes, diabetes, head trauma, brain tumors, and finally, coagulation disorders.
Alright, now let’s look at the pathology of hemorrhagic stroke, which can differ quite a bit depending on the underlying cause. With aging, hypertension, and diabetes mellitus, blood vessel walls are gradually affected by hyaline arteriolosclerosis, which is when various blood proteins get deposited in the walls, causing them to become more stiff, brittle, and therefore, more vulnerable to rupture. When this affects the small cerebral arteries, it can cause microaneurysms, or Charcot-Bouchard aneurysms. On the other hand, when aneurysms occur in bigger cerebral vessels, they are called cerebral aneurysms, which are typically congenital. With both types of aneurysms, the dilated portion of the blood vessel wall is structurally weaker and more prone to rupture.
Another source of the bleeding can be an arteriovenous malformation, which is a tangled blood vessel that directly connects an artery to a vein. Finally, intracerebral hemorrhage can result from hemorrhagic transformation of an ischemic stroke. See, with ischemic strokes, there’s a blockage of an artery that leaves the downstream tissue deprived of oxygen-rich blood. This results in brain tissue death, but also the death of endothelial cells of local blood vessels. So, when the blood flow to the affected part of the brain is restored, damaged blood vessels might rupture and eventually cause an intracerebral hemorrhage.
Now, hemorrhagic strokes can be further divided into two types: intracerebral hemorrhage, which occurs when there is bleeding within the cerebrum; and subarachnoid hemorrhage, which occurs when there is bleeding within the subarachnoid space.
With intracerebral hemorrhage, once the arterial blood vessel ruptures, blood pools within the skull and puts direct pressure on nearby tissue and blood vessels. Depending on where the bleeding occurs, intracerebral hemorrhage can be intraparenchymal, meaning within the brain tissue; or it can be intraventricular, when it occurs or extends into the brain ventricles. Now, as a result of bleeding, there’s less blood flowing downstream, leaving the tissue below the rupture deprived of oxygen-rich blood. Ultimately, this results in ischemia and neuronal dysfunction. Additionally, the pooling of blood is followed by local inflammation and edema, which further increases the intracranial pressure.
With subarachnoid hemorrhages, or SAH, on the other hand, blood accumulates within the subarachnoid space, eventually increasing the intracranial pressure and causing irritation of the meninges. Moreover, the breakdown of blood products within the subarachnoid space can result in narrowing of the cerebral arteries and subsequent ischemia of the brain tissue. This is called delayed cerebral ischemia or DCI for short.
Finally, the most important complications of hemorrhagic strokes include seizures, hydrocephalus, brain herniations, as well as rebleeding, hyperglycemia; hyponatremia; and venous thrombotic events, such as deep vein thrombosis and pulmonary embolism.
Hemorrhagic stroke can also lead to cardiac complications, such as arrhythmias, myocardial infarction, or heart failure, and pulmonary complications, like aspiration, pneumonia, or neurogenic pulmonary edema.
Now, the clinical manifestations of intracerebral hemorrhages are progressive, meaning that they develop over time; and they depend on the part of the brain that is affected. For example, a right anterior or middle cerebral artery stroke can cause numbness and sudden muscle weakness in the left part of the body, accompanied by disorientation and personality changes, such as poor judgment or impulsivity. In some cases, clients with a right-sided stroke can even be unaware of their deficit. Conversely, with a left anterior or middle cerebral artery stroke, the right side of the body will be affected.
An important thing to note is that an anterior cerebral artery stroke typically affects the feet and legs; while a middle cerebral artery stroke affects the hands, arms, face, and the language centers in the dominant hemisphere.
When the Broca’s area is affected there’s expressive aphasia where the client can understand what’s being said or written, but cannot produce complete sentences to express themselves. For example, they might say “taco taco table,” instead of “there are two tacos on the table.” Receptive aphasia occurs when the Wernicke’s area is affected, the client cannot understand spoken or written words, but they can produce speech resembling complete sentences that’s often meaningless. So they might say something like “I know but with the he came to Tuesday not before I showed him.”
On the other hand, a posterior cerebral artery stroke primarily affects the visual cortex, which affects a person’s ability to see clearly. Finally, if a stroke affects the cerebellum, it can cause a loss of balance or coordination.
In general, a useful acronym to remember some common stroke symptoms is BE FAST: balance impairment, eye symptoms like double vision or blindness, facial drooping, arm weakness, speech difficulties, and T is for time to call 911 which is not a symptom, but it’s a reminder to get help quickly and minimize cell injury and maximize the chance of a full recovery.
On the other hand, clinical manifestations of subarachnoid hemorrhage are acute, and the most prevalent feature is a sudden severe headache, often referred to as “thunderclap headache”. Other important features of subarachnoid hemorrhage include photophobia, or light sensitivity, and nuchal rigidity, which refers to a stiff neck caused by blood that is irritating the meninges.