Gonorrhea and chlamydia: Nursing process (ADPIE)
Client Report0:00–0:27
Chad Davis is a 22-year-old male who presents to the health department's sexually transmitted infection clinic with symptoms of painful urination and urethral discharge for the past 2 days.
Pathology0:27–4:06
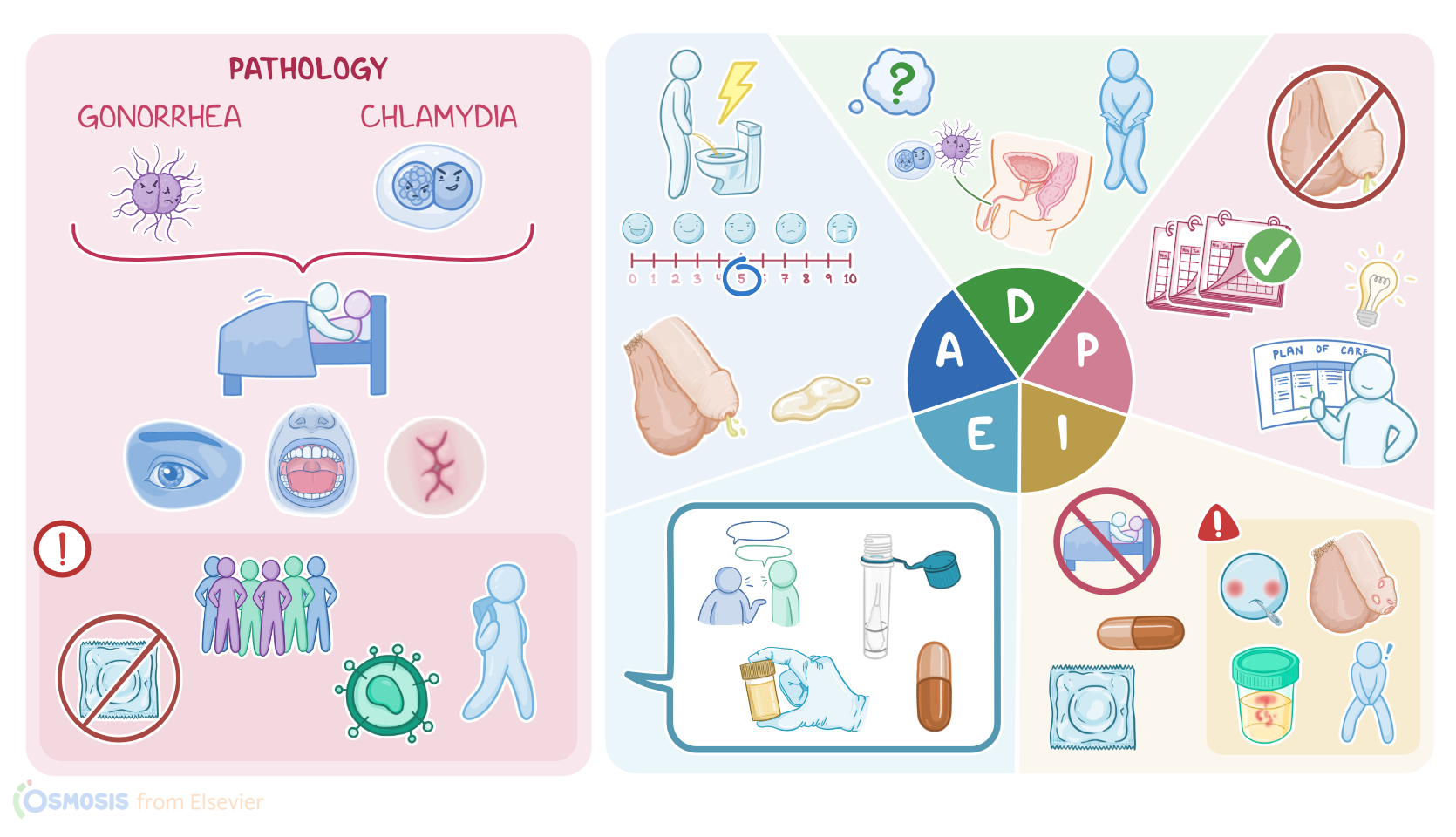
Gonorrhea and chlamydia are among the most common sexually transmitted infections, or STIs in the United States in both men and women.
Now, gonorrhea is caused by a gram-negative bacterium called Neisseria gonorrhea, while chlamydia is caused by a gram-negative bacterium called Chlamydia trachomatis.
Both infections are transmitted during sexual contact through sexual fluids, such as vaginal secretions or semen, so they often occur together, primarily affecting genital organs.
However, it's important to note that these infections can also be transmitted via contact with skin or mucous membranes, including eyes, mouth, and anus.
Risk factors associated with gonorrhea and chlamydia can be subdivided into two main groups. Behavioral risk factors include having unprotected sexual contact, as well as new or multiple sexual partners.
On the flip side, individual risk factors include young age, between 15 and 24 years old, since they're more likely to have new or multiple sexual partners, as well as having a history of prior sexually transmitted infections and HIV positive status.
Most often, gonorrhea and chlamydia cause asymptomatic infection. However, symptomatic clients can present with mucopurulent discharge from the vagina or penis, as well as dysuria or pain and burning during urination and urinary frequency.
In males, gonorrhea and chlamydia can infect the urethral mucosa, causing inflammation known as urethritis. Sometimes the infection can spread to the prostate, resulting in prostatitis.
Also, it can cause inflammation of the epididymis or epididymitis and cause symptoms such as testicular pain and swelling.
In females, there can also be urethritis, but typically, chlamydia affects the lower genital tract, causing vulvovaginitis, where the vulva and the vagina are affected, and cerviciis, where the cervix is involved.
This may present with changes in vaginal discharge, intermenstrual bleeding, and bleeding after sexual activity. Now an important complication in females is pelvic inflammatory disease, which is when the infection spreads to the uterus, fallopian tubes, and ovaries.
Finally, if left untreated, gonorrhea and chlamydia can cause infertility in both male and female clients. Diagnosis of gonorrhea and chlamydia starts with history and physical examination and can be confirmed with nucleic acid amplification testing or NAAT, which uses a genital swab or urine sample to look for the bacterial DNA.
Treatment of gonorrhea and chlamydia requires the administration of antibiotics. Gonorrhea is usually treated with a 3rd generation cephalosporin called ceftriaxone, while chlamydia can be treated with macrolides like azithromycin or tetracyclines like doxycycline.
As you enter the room, you begin your assessment by asking questions about Mr. Davis's sexual health history.
Assessment4:06–6:03
On visual inspection, his sclera appears white and free of conjunctivitis. His oral and pharyngeal mucosa are moist, pink, and without lesions, and his skin is intact without rashes or lesions.
Heart sounds are normal and lungs are clear. Bowel sounds are active, and Mister Davis reports no changes in his appetite, nausea, or vomiting.
Next, you assess his genital region and note the absence of lesions, inguinal lymph node swelling, and testicular swelling.
Penile swelling is present along with a thick, cloudy, white, foul smelling discharge oozing from his urethra. Mr.
Davis states he has felt the urge to void more frequently and experiences pain during urination. His rectum is free of lesions, swelling, and bleeding, and he denies rectal pain or changes in bowel movements.
His vital signs are oral temperature 98.8 °F or 37.1 °C. Heart rate 75 BPM, respirations, 16 breaths per minute.
BP 118/72 millimeters of mercury, SPO2, 100% on room air, and current pain score is 0 out of 10, but 5 out of 10 while urinating.
You document your assessment findings before leaving the room. Your nursing diagnoses include infection related to unsafe sexual practices, acute pain related to arthritis, impaired urinary elimination related to your arthritis, and deficient knowledge related to chlamydia treatment and prevention.
Diagnosis6:03–6:18
With the interdisciplinary team, you plan goals of care for Mr. Davis.
Planning6:18–6:50
By the end of today's visit, Mr. Davis will verbalize understanding of chlamydia transmission, treatment, and prevention.
Additionally, Mr. Davis will test negative for infection at his 3-month follow-up.
All right, now it's time to implement your interventions to help Mr. Davis meet his goals.
Implementation6:50–8:29
Davis will be treated for presumed chlamydia with a single dose of the antibiotic azithromycin. After collecting the ordered labs, you administer the azithromycin.
Next, you begin teaching Mr. Davis about chlamydia, how it is transmitted, and that the antibiotic is needed to resolve the infection and improve his symptoms.
You advise Mister Davis to seek medical attention if he experiences new abdominal or pelvic pain, fever, has difficulty urinating or has blood in his urine, develops scrotal pain or swelling, has new or worsening penile discharge, or develops skin lesions in the genital or anal area.
You emphasize that both Mr. Davis and his partner should abstain from sexual contact for 7 days after completing treatment, and that they should return to the clinic to be retested in 3 months.
As you explain how STIs are transmitted and how using condoms with each sexual encounter reduces risks of infection, you also discuss the importance of talking with sexual partners regarding risks and routinely screening for STIs when engaging in risky sexual behavior like being in a non-monogamous relationship.
Before leaving the exam room, you document the nursing interventions provided. Now it's time to evaluate nursing interventions provided to Mr.
Evaluation8:29–9:18
Davis during today's visit. The antibiotic azithromycin was administered to treat chlamydia, which should also resolve his symptoms.
When his lab results are back, you will collaborate with the interdisciplinary team to determine if further interventions are needed.
By adhering to the education you provided, you are hopeful Mr. Davis will test negative for infection when he returns to the clinic in 3 months.
Summary9:18–10:14
All right, as a quick recap, Mr. Davis was treated for chlamydia at the health department's STI clinic.
Chlamydia is a common STI caused by the bacteria Chlamydia trachomati and is transmitted during sexual contact. Your nursing assessment revealed Mr.
Davis was experiencing dysuria, penile swelling, and penile discharge. Your nursing diagnoses included infection, acute pain, impaired urinary elimination, and deficient knowledge.
His plan of care included testing for STIs, administering an antibiotic, and providing thorough education about chlamydia treatment, transmission, and prevention.
Together with the interdisciplinary team, you implemented the strategies to help Mr. Davis reach these goals.
You will continue to evaluate his response to your interventions and adjust the plan of care as needed.
| GONORRHEA AND CHLAMYDIA | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Pelvic Inflammatory Disease Due to Neisseria gonorrhoeae and Chlamydia trachomatis: Immune Evasion Mechanisms and Pathogenic Disease Pathways" J Infect Dis (2021)
- "An Update on Gonorrhea and Chlamydia" Obstet Gynecol Clin North Am (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Screening for Chlamydia and Gonorrhea" JAMA (2021)
- "Etiology and Diagnosis of Pelvic Inflammatory Disease: Looking Beyond Gonorrhea and Chlamydia" J Infect Dis (2021)
- "Screening for chlamydia and/or gonorrhea in primary health care: systematic reviews on effectiveness and patient preferences" Syst Rev (2021)
No notes for this video yet
Try adding a note below