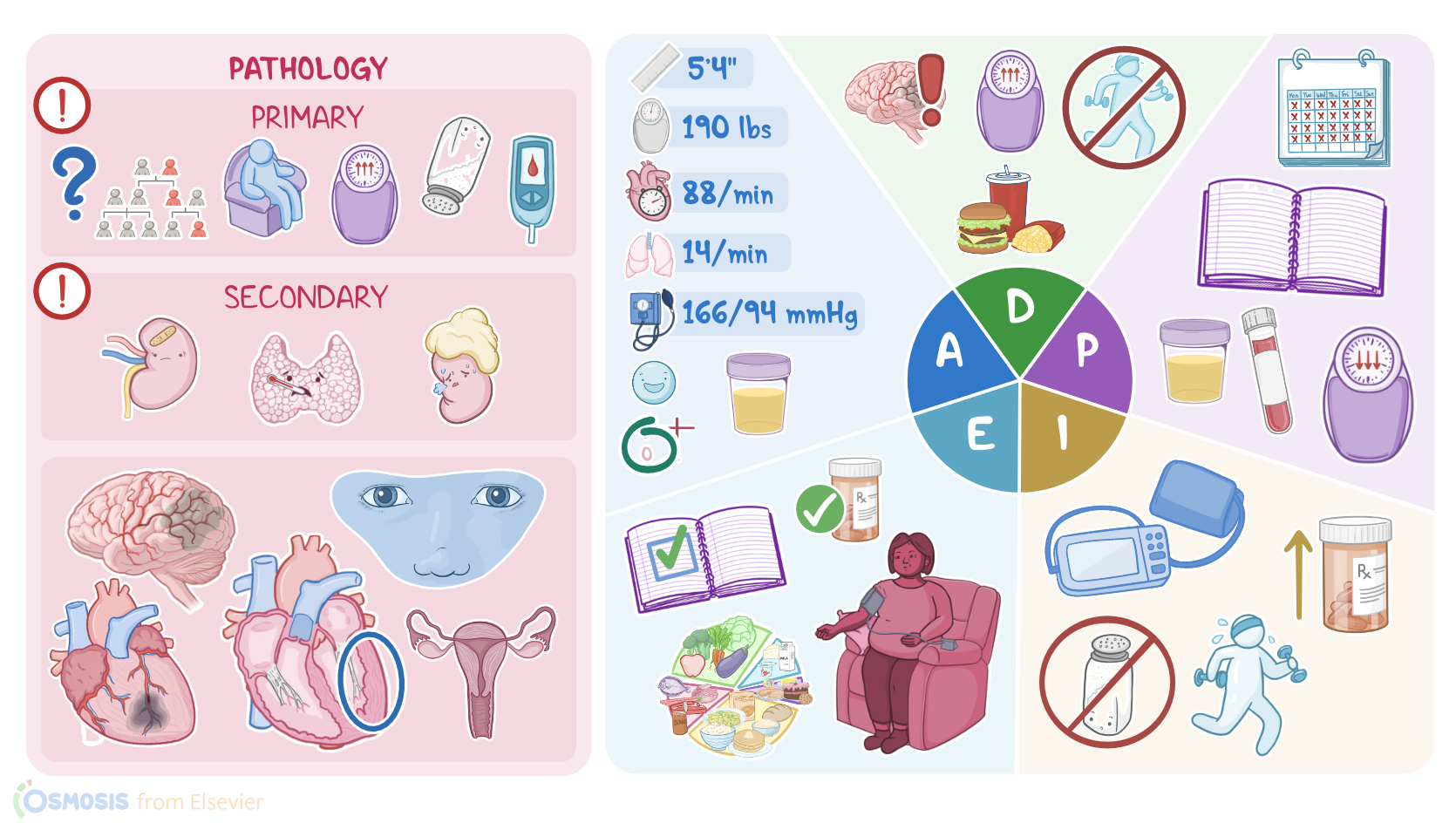
Hypertension: Nursing process (ADPIE)
3,236views
Hypertension: Nursing process (ADPIE)
Cardiovascular MedSurg
Cardiovascular MedSurg
Notes
| HYPERTENSION | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Jada Williams is a 55-year-old African American female who presents to her primary care office.
At her visit one month ago, her blood pressure was 150/94 mmHg.
She was diagnosed with stage 2 hypertension and started on blood pressure medication.
Hypertension, commonly referred to as high blood pressure, is a very common condition, impacting about 1 billion people around the world.
Blood pressure is classified in five categories: normal, elevated, stage 1, stage 2, and hypertensive crisis.
Blood pressure is considered normal when the systolic blood pressure is more than 90 mmHg but less than 120 mmHg and the diastolic blood pressure is more than 60 mmHg but less than 80 mmHg.
When the systolic blood pressure is between 120 and 129 mmHg and the diastolic blood pressure is less than 80 mmHg, the blood pressure is said to be elevated.
Stage 1 hypertension is between 130 and 139 mmHg on the systolic side, and between 80 and 89 mmHg on the diastolic side.
Stage 2 hypertension is defined as anything that is 140 mmHg or higher on the systolic side and 90 mmHg or higher on the diastolic side.
Hypertensive crisis is present when the systolic blood pressure is over 180 mmHg or the diastolic blood pressure is over 120 mmHg.
Now, there are also two types of hypertension, primary hypertension, which accounts for about 90 percent of hypertension cases, and secondary hypertension, which is much less common.
Primary hypertension has no known underlying cause, but it is thought to be due to the interaction of environmental and genetic factors affecting the cardiovascular and renal systems.
Several risk factors contribute to primary hypertension.
For example, nonmodifiable risk factors include advanced age, biological male sex, a family history of hypertension, diabetes mellitus, and African American or Hispanic ethnicity.
Modifiable risk factors include a sedentary lifestyle, obesity, smoking, excess sodium and alcohol consumption, and stress.
On the other hand, secondary hypertension is caused by an underlying medical condition that elevates blood pressure, such as kidney disease, thyroid dysfunction, or adrenal disorders.
Clients with hypertension often won’t have any symptoms, and this is why hypertension is known as the silent killer.
In some cases, however, high blood pressure can damage blood vessels in the heart, brain, kidneys, eyes, reproductive organs and peripheral arteries, causing symptoms such as headache, dizziness, visual changes, and chest pain.
Left untreated, hypertension can result in myocardial infarction, stroke, kidney disease, vision loss, sexual dysfunction, aortic dissection, and peripheral artery disease.
Furthermore, hypertension increases afterload, which is the amount of pressure the heart needs to work against to eject blood.
This increases the workload of the heart, eventually causing enlargement and thickening of the heart muscle and complications such as heart failure.
Now, let’s talk about how hypertension is diagnosed.
In order to increase accuracy before making a diagnosis, blood pressure should be measured at least two times on two separate occasions and proper technique should be followed.
The client should rest for at least five minutes, sitting with feet on the floor, back supported, and arm supported at the level of the heart.
The blood pressure cuff should fit properly and should not be placed over clothing.
Before measurement, the client should avoid anything that might increase their heart rate, like smoking or caffeine, at least thirty minutes prior to blood pressure measurement.
Once hypertension is diagnosed, the client should be assessed for signs of complications from hypertension with tests such as a lipid profile, kidney function panel, urinalysis, electrocardiogram, and ophthalmic exam.
A complete blood count, fasting glucose, thyroid stimulating hormone, kidney function panel, and urinalysis may be ordered to check for conditions causing secondary hypertension.
Treatment is focused on lifestyle modifications and pharmacological interventions.
The goal of treatment is to reduce blood pressure and reduce the risk of complications.
The Dietary Approaches to Stop Hypertension diet, referred to as the DASH diet, is recommended to reduce dietary sodium and help clients achieve a healthy weight.
Exercise, smoking cessation, limiting alcohol and caffeine, and reducing stress are also important lifestyle changes needed for hypertension control.
Eliminating unnecessary substances like recreational drugs that can raise blood pressure is important too.
Pharmacological interventions are based on each client’s individual needs.
The four primary drug classes to treat hypertension include thiazide diuretics such as hydrochlorothiazide; angiotensin converting enzyme inhibitors; or ACE inhibitors, like lisinopril; angiotensin II receptor blockers or ARBs, such as losartan; and calcium channel blockers, or CCBs, like amlodipine.
All right, back to your client Ms. Williams.
You call Ms. Williams into the exam room, introduce yourself as her nurse, confirm her identity, and begin your assessment.