Hypospadias and epispadias: Nursing
Hypospadias and epispadias: Nursing
Nicu
Nicu
Notes
| HYPOSPADIAS AND EPISPADIAS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
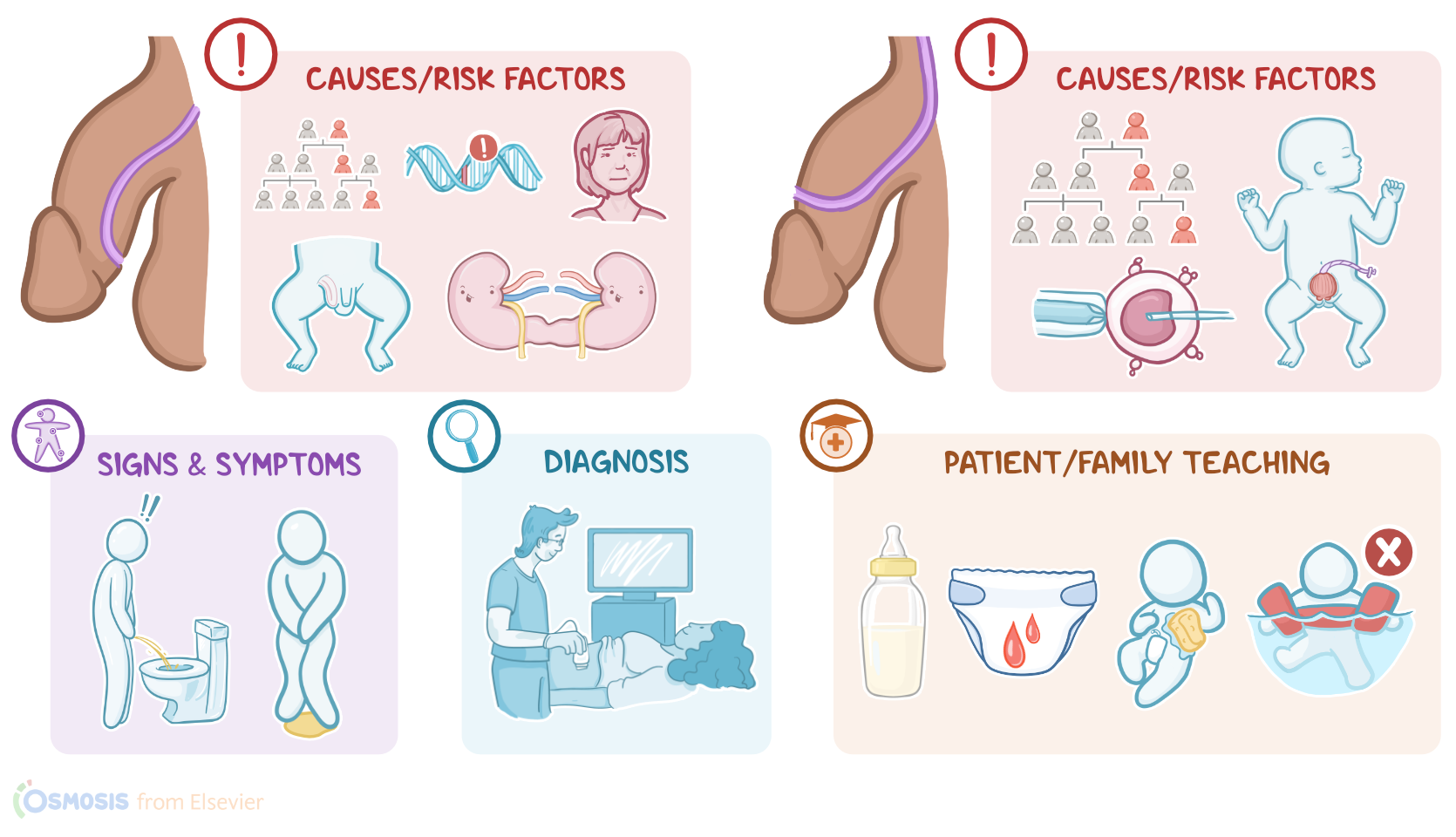
Hypospadias and epispadias are congenital conditions associated with an abnormal position of the urethral opening. In hypospadias, the urethral opening is located along the underside of the penis, on its ventral surface; while in epispadias the urethral opening is positioned along the upper side of the penis, on its dorsal surface.
First, let’s cover some basic physiology and embryology of the male external genitalia. Around the 8th week of pregnancy, the testes start to produce testosterone, which is an androgen responsible for masculinization of the external genitalia. So, in the genital tubercle, urogenital sinus, urogenital folds, and labioscrotal swellings, testosterone is converted to a more potent form called dihydrotestosterone or DHT for short.
Dihydrotestosterone elongates the genital tubercle in the cranial direction, meaning towards the future head, into a primitive phallus, which represents the precursor of the future penis. In the urogenital sinus, it stimulates the formation of the bladder, prostate, bulbourethral glands, and the part of the urethra outside of the penis. On the flip side, in the urethral folds, it stimulates the formation of the ventral shaft of the penis and the penile urethra. Finally, dihydrotestosterone makes the urethral folds and the labioscrotal swellings fuse on the midline in order to form the ventral shaft of the penis, the penile urethra and the scrotum, respectively.
Now, the exact cause of hypospadias and epispadias is still unknown, but some theories suggest they might be associated with abnormal levels of androgens and estrogens. Important risk factors for hypospadias include family history, genetic mutations, maternal age over 35 years, maternal hypertension or diabetes, and maternal exposure to tobacco smoke or pesticides.
Additionally, clients with some congenital conditions have a higher incidence of hypospadias than others. These include inguinal hernia; which occurs when an internal organ, like intestines, protrudes through the inguinal canal; cryptorchidism, which refers to the absence of one or both testes from the scrotal sac; and chordee, or abnormal downward or upward curvature of the penis. Hypospadias is also associated with renal congenital malformations, like renal agenesis, or the absence of one or both kidneys; horseshoe kidney, or fused kidneys; or ureteropelvic junction obstruction.
On the flip side, important risk factors for epispadias include family history, and assistive reproductive technologies, or ARTs for short. Epispadias can also be associated with a congenital abnormality, called bladder exstrophy, which is where the bladder protrudes outside of the abdomen due to an abdominal wall defect.
Now, pathology-wise, in clients with hypospadias, the urethral folds fail to meet up and close adequately, eventually leaving the urethral opening along the ventral side of the penis. Based on the location of the urethral opening, hypospadias can be defined as glanular, or near the head of the penis; midshaft, or located in the middle of the penis; and penoscrotal, at the penis root, where the penis and scrotum come together.
On the other hand, clients with epispadias have a malpositioned genital tubercle that grows towards the rectal area instead of the head. Based on the location of the urethral opening, epispadias can be defined as glanular, or near the head of the penis; penile, or located along the penile body; and penopubic, which are found at the root of the penis. Finally, both hypospadias and epispadias can cause serious complications like erectile dysfunction and infertility.
Alright, let’s switch gears and discuss clinical manifestations. Clients with hypospadias present with an abnormal urethral opening along the ventral surface of the penis. On the other hand, clients with epispadias present with an abnormal urethral opening along the dorsal surface of the penis. Other important clinical manifestations of hypospadias and epispadias include problems when aiming the stream of urine and urinary incontinence.
Diagnosis of hypospadias and epispadias is based on the client’s history, physical assessment and detection of an abnormal urethral opening along the ventral or dorsal surface of the penis. Prenatal diagnosis is also possible via an ultrasound, which usually shows a small, blunted penis. An ultrasound is also useful for detecting other anomalies commonly associated with hypospadias such as cryptorchidism, or other urologic malformations.
Treatment of hypospadias and epispadias requires surgical reconstruction of the urethra. This is indicated within the first 2 years of life and includes closure of the abnormal urethral opening and opening of the new one on the tip of the glans. A surgeon can use the foreskin to reconstruct the urethra, therefore circumcision should not be performed in clients with hypospadias or epispadias. After the reconstruction, some clients might present with postoperative complications like meatal stenosis, or stenosis of the urethral opening, urethral strictures, and subsequent obstruction of the urine flow.
Okay, when caring for a client with hypospadias, your priority goals of nursing care are to provide postoperative care and monitor for complications. Now, when providing postoperative care for your client, provide routine care and monitor for complications related to the procedure. There will be a catheter in place to allow for drainage of urine, so be sure to check that it's correctly taped with the penis in an upright position, which will prevent stress on the incision. Encourage fluid intake to promote flow of urine, which will help prevent occlusion of the catheter; and closely monitor the amount of urine output. Report to the healthcare provider if there is no urine output for one hour, as this could indicate the presence of an occlusion.