Infant of a diabetic mother (IDM): Nursing
Infant of a diabetic mother (IDM): Nursing
Medical Surgical
Medical Surgical
Notes
| INFANT OF A DIABETIC MOTHER | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Infants of mothers with diabetes, or IDMs for short, have a higher risk of developing fetal and neonatal complications, including growth abnormalities, respiratory distress, and metabolic complications, in addition to preterm delivery.
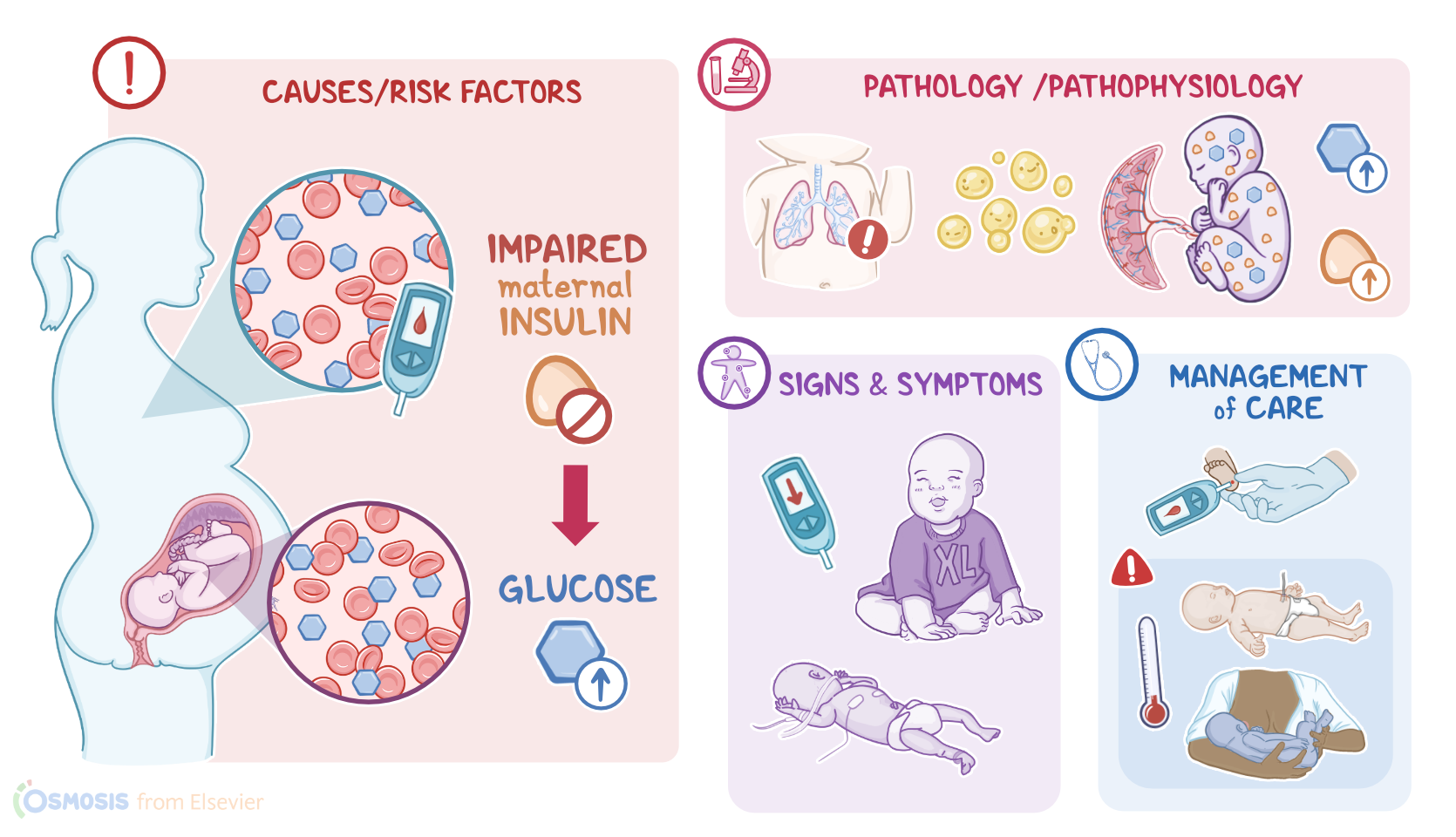
Alright, let’s take a look at the physiology of glucose metabolism during pregnancy. During fetal development, all of the nutrients the fetus receives come directly from the mother's blood through the placenta. Glucose is the primary source used by the fetus for growth and development. Fetal insulin reduces blood glucose by binding to insulin receptors embedded in the cell membrane. When activated, the insulin receptors allow glucose to be transported into the cell, thereby moving glucose from the blood and into the tissues. During pregnancy, hormones released by the placenta increase the mother’s body’s resistance to insulin, resulting in higher levels of maternal blood glucose. These metabolic changes allow the fetus to receive a steady supply of glucose necessary for fetal growth and development.
Now, diabetes occurs when the body’s ability to produce or respond to the hormone insulin is impaired, resulting in higher blood glucose levels. Diabetes in pregnancy can be either pregestational, which is where diabetes is diagnosed before pregnancy; or gestational, which is where mothers without previously diagnosed diabetes have high blood glucose levels during pregnancy, especially during their third trimester. The risk of fetal and neonatal complications increases with higher maternal glucose levels or BMI.
Now, pathology-wise, poor glucose control at the time of conception and during the first trimester can interfere with organogenesis in the embryo, resulting in major birth defects and spontaneous abortions early in pregancy; and this most common with pregestational diabetes, because blood glucose is more likely to be elevated around the time of conception and during the first trimester when the fetal organs are being formed. On the other hand, with gestational diabetes, glucose control isn’t usually impaired until the second or third trimester. By that time, fetal organs are almost fully developed and congenital birth defects are much more rare.
Now, regardless of the type of diabetes, large amounts of glucose from the mother are transferred to the fetus.
Unlike glucose, maternal insulin does not cross the placental barrier, so the excessive glucose in the fetal blood signals the fetal pancreas to release more and more insulin, resulting in hyperinsulinemia.
High levels of insulin interferes with normal lung development and decreases surfactant production. Hyperinsulinemia also increases the metabolic rate of the fetus which increases the need for oxygen, increasing the risk of fetal hypoxia. Hypoxia stimulates erythropoiesis, increased production of RBCs, which ultimately leads to polycythemia.
The excess glucose in the fetal blood also increases fat deposits in the subcutaneous tissues and other organs like the liver, heart, and muscle. This causes the fetus to grow much larger than normal, resulting in neonatal macrosomia, meaning that the newborn weighs 4,000 g or more. On the flip side, mothers who have diabetic-related vascular disease tend to have poorly functioning placentas, and this results in placental insufficiency, which means the flow of oxygen-rich blood through the placenta and to the developing fetus is impaired, resulting in intrauterine growth restriction, or IUGR for short.
Now, after delivery, the newborn’s insulin level remains high, but the supply of glucose is abruptly cut off when the umbilical cord is cut. So, the most common complication in the neonatal period is hypoglycemia.
Other complications include birth injuries due to macrosomia, since the larger body size makes vaginal delivery more difficult, and increases the risk for trauma during birth, including brachial plexus or facial nerve injury, clavicular or humeral fractures, cephalohematoma, or subdural hemorrhage. Respiratory distress is a common complication due to lung immaturity; as well as polycythemia-related problems like hyperbilirubinemia caused by the breakdown of an increased number of circulating red blood cells; as well as hyperviscosity, which can lead to a sluggish blood flow, ischemia, and thrombosis of vital organs. There are also complications related to congenital birth defects like heart or neural tube defects; and lastly, infants of diabetic mothers are at increased risk of preterm delivery and associated complications.
Alright, in terms of clinical manifestations, most infants of mothers with diabetes have a macrosomic appearance, with a round puffy face, plethoric or ruddy skin, a larger body, and a higher than normal birth weight. On the other hand, infants with IUGR typically present with low birthweight, decreased subcutaneous fat and muscle mass, and a thin umbilical cord.
Now, in cases where there’s newborn hypoglycemia, clinical manifestations may include irritability, jitteriness, lethargy, difficulty feeding, and seizures. In the case of hyperbilirubinemia, the infant’s skin and mucous membranes can take on a yellowish color, a condition known as neonatal jaundice. Finally, newborns with impaired lung development may exhibit signs of respiratory distress, like tachypnea, respiratory retractions, and nasal flaring shortly after birth.
Alright, the diagnosis of infants of mothers with diabetes starts with prenatal history and physical assessment of both mother and baby. During pregnancy, maternal blood glucose levels and intrauterine fetal growth is part of the diagnosis.