Lyme disease: Nursing process (ADPIE)
Lyme disease: Nursing process (ADPIE)
Medical Surgical
Medical Surgical
Notes
| LYME DISEASE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
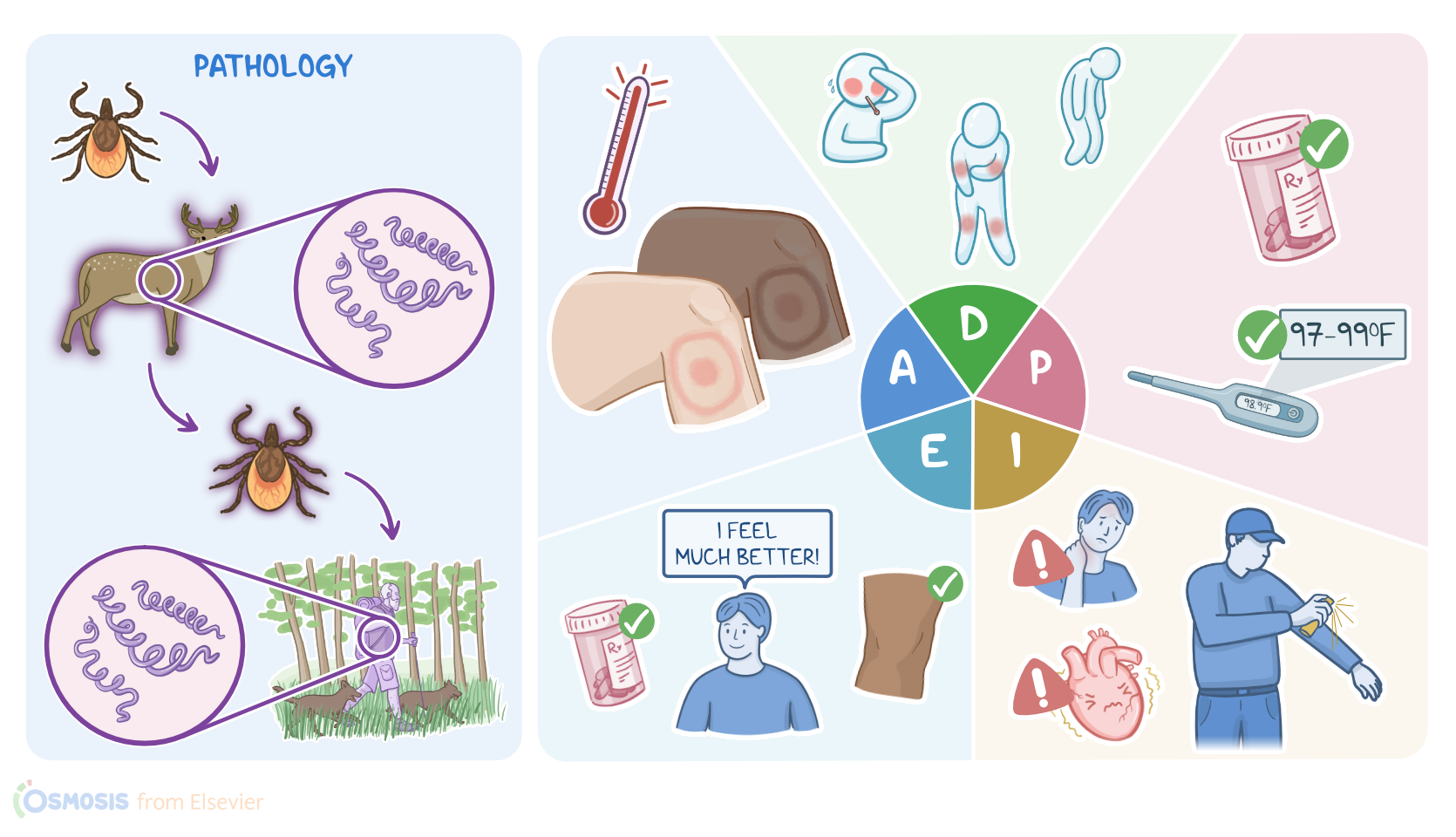
Jacob Myers is a 32-year-old male who presents to his primary care provider after discovering a painless bulls-eye looking rash on his thigh that has gotten bigger over the past three days.
He also reports symptoms of fatigue, fever, chills, muscle aches along with joint pain and stiffness that started three days after he returned from a week-long camping trip.
The provider suspects that Jacob has Lyme disease. Lyme disease is an infectious disease that’s caused by a bacterial species called Borrelia, most often Borrelia burgdorferi.
The Borrelia species are all spirochetes, which means that they are long, thin, and spiral-shaped.
Now, Lyme disease is a zoonotic disease, meaning that it can infect a wide range of animals, including deer, cattle, and rodents, but it isn’t known to spread directly from animals to humans, but instead it needs a vector, meaning some sort of intermediate organism to spread from the animal to the human.
In Lyme disease, the vector is the Ixodes tick, which is often found in wooded areas, thick brush, marshes, and tall grass.
Now, the transmission of Lyme disease starts when the Ixodes tick feeds on the blood from an infected animal host.
If this tick then feeds on the blood from a human, it will transmit the bacteria with their saliva.
Once the bacteria is in a human's bloodstream, it can disseminate to distant tissues, particularly the skin, joints, and heart, causing inflammation and damage.
Now, there are some factors that may put a client at risk of Lyme disease, such as outdoor activities in wooded or grassy areas, like hiking and hunting, as well as some occupations like landscaping, farming, and railroad work.
The risk is also increased when clients wear clothing that exposes the skin. In addition, Lyme disease is more common during spring and summer, as ticks typically prefer warm temperatures.
Now, symptoms of Lyme disease can progress through three stages. The first is called the early localized stage, which starts within 1 month of the tick bite.
Clients in this stage might report flu-like symptoms like fever, headache, fatigue and lymphadenopathy, as well as muscle or joint pain.
A characteristic symptom of the early localized stage of Lyme disease is erythema migrans, which is a painless, red skin lesion that slowly expands over a few days around the site of the tick bite, developing a bulls-eye shape.
Now, if the disease is not treated at its first stage, the bacteria can disseminate to places like the joints, heart, and brain.
The second stage of Lyme disease is the early disseminated stage which usually occurs within weeks to months from the initial infection, and can cause complications like arthritis, most often involving the knees, wrists, and ankles.
This is called transient migratory arthritis, which is when arthritis resolves in one joint and moves to affect another.
Another complication at this stage is carditis, or inflammation of the heart, which increases the risk for arrhythmias, such as atrioventricular block, where electrical impulses can’t pass from the atria to the ventricles.
Finally, the early disseminated stage can also cause neurological complications like meningoencephalitis and facial nerve palsy, where there’s a weakness on one side of the face.
Ultimately, clients can reach the third stage of Lyme disease, also called the late disseminated stage, which usually develops months or sometimes even years after the initial infection.
The third stage typically presents with chronic arthritis, as well as neurological manifestations like chronic encephalopathy, gait abnormalities, fatigue, memory loss, and personality changes.
Finally, the third stage of Lyme disease can cause damage to peripheral nerves, which manifests as pain, numbness, and muscle weakness mainly involving the limbs.
Now, diagnosis of Lyme disease is typically based on history and physical examination.
Diagnosis can be confirmed with blood tests, which look for antibodies against Borrelia.
This starts with enzyme-linked immunosorbent assay, or ELISA, and is then confirmed with Western blot.