Migraines: Nursing
Notes
| MIGRAINES | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Migraines are a specific type of recurrent headache that’s characterized by moderate to severe pulsating or throbbing pain, which is typically localized to one side of the head, and can be very disabling.
Okay, first, a bit of physiology. The cells that make up our brain are called neurons, and have three main parts, the dendrites, cell body, and axon. The dendrites are little branches that receive signals from other neurons, and carry them to the cell body, which has all of the neuron’s main organelles. The cell body then transmits the signal through the axon, which ultimately releases neurotransmitters in order to send the signal along to the dendrite of another neuron. Depending on the signal, the result is either the excitation or inhibition of that neuron.
Now, normally, throughout the body, there are special neurons that act as pain receptors, called nociceptive nerve fibers. When these neurons detect a painful stimulus, they send a signal that conveys the feeling of pain to the brain. The brain itself does not have pain receptors, but it can detect signals from pain receptors of nearby tissues in the head and neck, such as the blood vessels, muscles, and the meninges covering the brain.
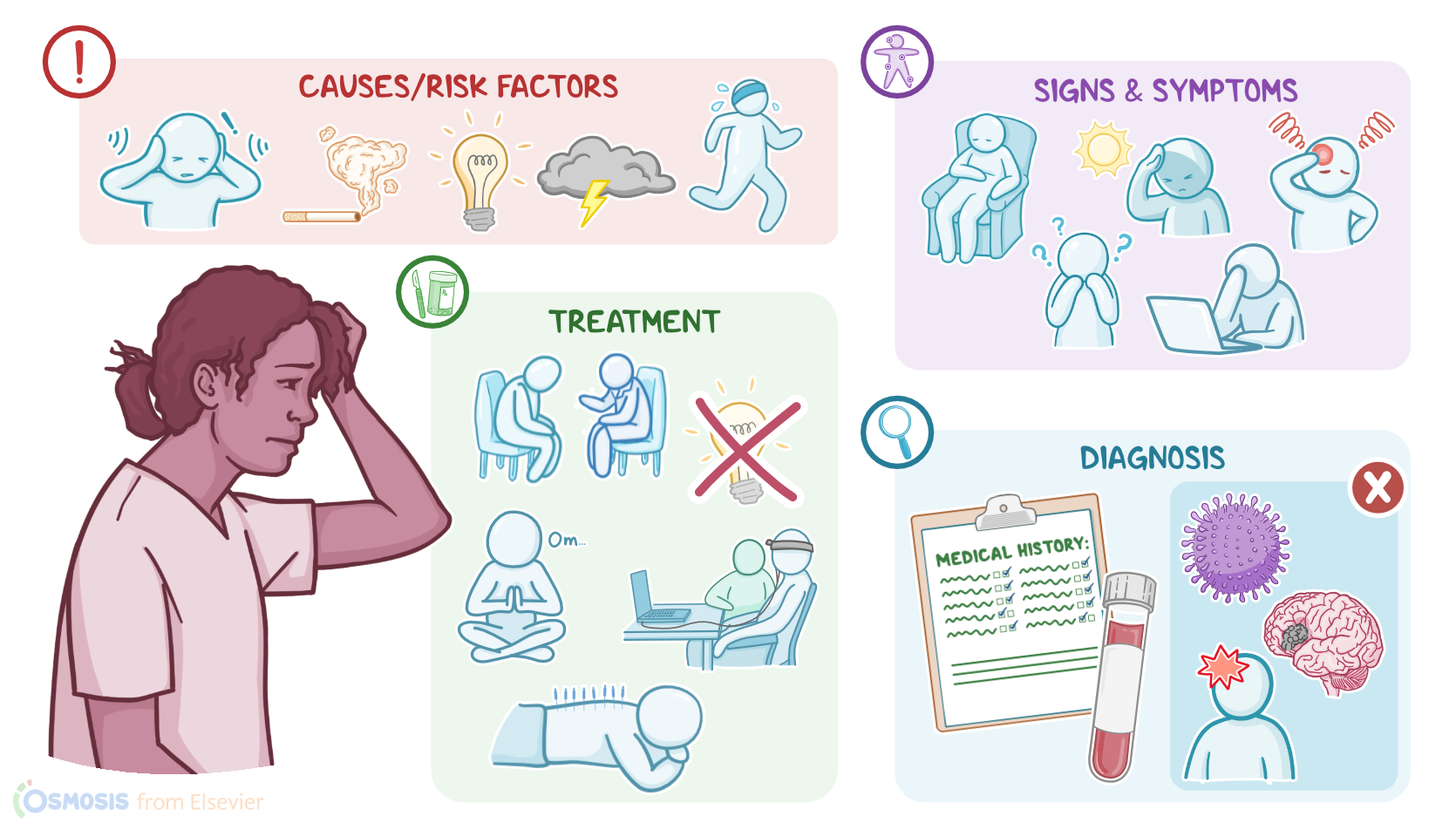
Although the underlying cause of migraines isn’t well understood, it seems to be related with neuronal hyperexcitability, where neurons respond excessively to a signal. The main risk factors include family history, an age between 25 and 55 years, and being assigned female at birth. Other risk factors include obesity, depression, and emotional or physical stress. In addition, migraine attacks are often associated with specific triggers, such as bright or flickering lights; loud noises; physical exertion; lack of sleep; weather changes; cigarette smoke; foods like chocolate or cheese, alcohol, especially red wine, as well as some food additives and the artificial sweetener aspartame; and medications like oral contraceptives. In young individuals, migraine attacks can be also triggered by hormonal shifts that occur during the menstrual cycle.
Okay, so in clients who experience migraines, neuronal hyperexcitability causes the brain to be hypersensitive to these triggers. This seems to abnormally activate the trigeminal nerve. As a result, the trigeminal ganglion releases vasoactive peptides like calcitonin-gene related peptide or CGRP for short, which in turn binds to receptors around meningeal vessels and causes them to dilate. This ultimately triggers neurogenic inflammation, which leads to a migraine attack. Now, migraine attacks are often preceded by prodrome or premonitory symptoms, which can begin hours to days before the headache itself, and include mood or sleep changes, poor concentration, fatigue, and irritability, as well as nausea, increased thirst, or cravings for foods high in salt, fat, or sugar.
Some clients can also experience an aura, usually within one hour before the onset of the headache, which is characterized by sensory disturbances like seeing flashing lights, zigzag lines, and blind spots, as well as tinnitus or ringing in the ears, and smelling strange odors. In addition, some clients may present with aphasia, confusion, paresthesia, or temporary paralysis of one side of the body.
Now, the migraine itself usually lasts between 4 to 72 hours, and feels like a progressive pulsating or throbbing pain, typically localized to one side of the head. As if this was not bad enough, these headaches tend to come with nausea or vomiting, irritability, and pain or discomfort with lights, sounds, and smells, respectively called photophobia, phonophobia, and osmophobia.
After a migraine attack is over, clients may experience postdrome symptoms, which can last a day or two, and include fatigue, difficulty concentrating, and feeling sore at the location of the pain.
Diagnosing a migraine is usually based on the client’s history and physical assessment. Sometimes, imaging and laboratory tests can be performed to rule out other conditions, such as an infection, brain tumor, stroke, or head injury.
Now, treatment of migraines aims at reducing the symptoms with abortive therapy, and typically includes over-the-counter analgesics, such as acetaminophen or NSAIDs like ibuprofen. Clients with severe pain or who don’t respond to these analgesics can be prescribed serotonin agonists, such as ergot derivatives like ergotamine, and triptans like sumatriptan, or calcitonin gene-related peptide or CGRP receptor antagonists like erenumab.
Now, clients that have very severe, debilitating migraines may benefit from preventive treatment, which aims at keeping the attacks from happening in the first place. Options include anticonvulsants like topiramate, beta blockers like metoprolol, calcium channel blockers like verapamil, or tricyclic antidepressants like amitriptyline, as well as CGRP receptor antagonists like erenumab. For adult clients, botulinum toxin A injections have also been shown to prevent migraines.