Hypersensitivity reactions - Type I: Nursing
Hypersensitivity reactions - Type I: Nursing
Medical Surgical
Medical Surgical
Notes
| HYPERSENSITIVITY REACTIONS - TYPE I | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
Transcript
A hypersensitivity reaction is an overreaction to a foreign antigen which then causes serious damage to the body’s tissues. There are four types of hypersensitivity reactions: type I is immunoglobulin E, or IgE mediated; type II is mediated by antibodies that activate cellular cytotoxicity, type III is mediated by immune-complexes, and type IV is a delayed T cell mediated hypersensitivity reaction. Type 1 hypersensitivity reactions, or IgE-mediated reactions, are an immediate immune response where the IgE antibody responds to an antigen, causing acute inflammation.
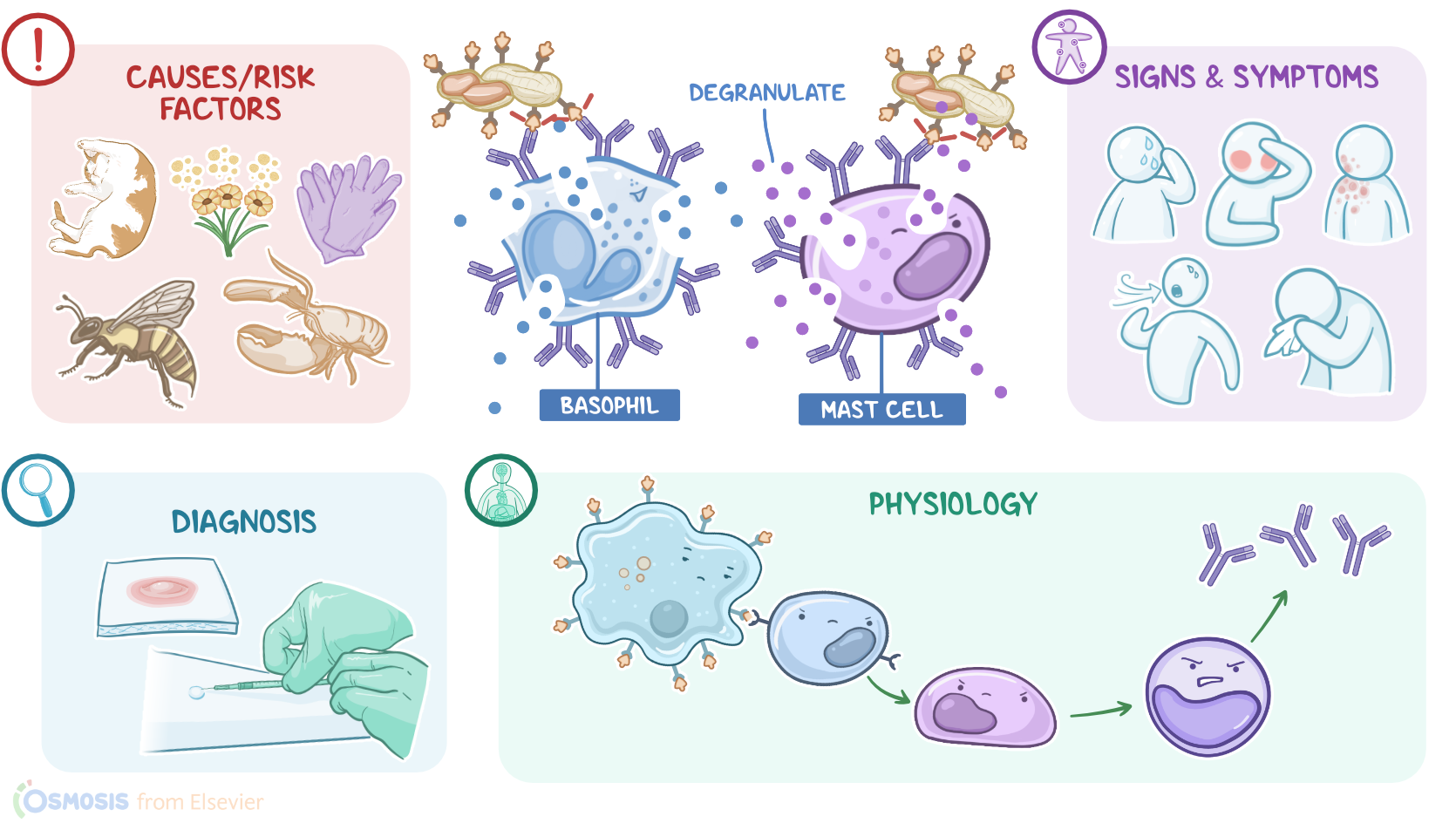
Let’s start by looking at the physiology of the immune response. A food allergen or pathogen enters the body and runs into antigen-presenting cells, or APCs. APCs like macrophages or dendritic cells, then engulf and digest the allergen and the fragments are then presented on the APC’s surface via proteins called major histocompatibility complex class II, or MHC II. Now these fragments serve as antigens which are any thing that could trigger an immune response. So the APCs present these antigens to T helper cells which have T-cell receptors, or TCRs, that recognize the antigen. In response, the T helper cells will signal B Cells to transform into plasma cells that will start producing antigen specific IgE antibodies.
These antibodies bind to other immune cells like mast cells and basophils and prep them to fight off the allergen in future encounters. This process is called priming or sensitization. So the next time the food allergen shows up, the mast cells armed with the IgE antibodies will use them to attach to the antigens on the allergen. When two or more of the antibodies on the mast cell bind to the antigen, it will cause the mast cell to degranulate and release various proinflammatory molecules. One of these is histamine which causes vasodilation, and increases blood vessel permeability. This increases blood flow to the area and lets other immune cells, like macrophages, get to the allergen. Meanwhile, other proinflammatory molecules released by mast cells such as interleukins and prostaglandins will attract more immune cells to the region.
Now, type I hypersensitivity reactions are caused by exposure to allergens, which are antigens that are normally harmless to the body, but still trigger a strong immune response. Common allergens include venom from bee stings, foods like peanuts or shellfish, inhaled airborne particles like pollen, pet dander, or dust, and some can cause a reaction through skin contact like a pet’s fur and saliva or latex gloves.
Now, for risk factors, the hygiene hypothesis considers that a very clean environment minimizes a child’s exposure to infections, germs, and allergens which puts them at greater risk of developing allergies later on, because their body didn’t have as many opportunities to build up tolerance to various non-harmful foreign substances. Many clients also have a genetic predisposition to develop allergies.
Okay, the pathological process of type I hypersensitivity begins with an initial exposure to an antigen, like pollen, which causes production of IgE antibodies that target the allergen. These will bind to and sensitize the mast cells and basophils. So on future exposures to the allergen, the mast cells bind to all the antigens that enter the body and degranulate, which means they release histamine and other proinflammatory molecules, causing inflammation, vasodilation, and vasopermeability. In addition, histamine also triggers smooth muscle contraction, and in the bronchus, it leads to narrowing of the airways.
All of this can happen within minutes to hours so type I hypersensitivity reactions are also called immediate reactions. Anaphylaxis is the more severe and systemic version of this process and leads to anaphylactic shock where the vasodilation and increased vasopermeability decreases the blood pressure so much that organs like the brain and heart are no longer sufficiently prefused.