Mood disorders: Nursing
Mood disorders: Nursing
NUR393
NUR393
Notes
| MOOD DISORDERS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Mood disorders are mental health conditions that affect a client’s emotional state, which can range from depression or extreme sadness to mania or excessive excitement.
Now, let’s go over some physiology. Emotions are processed in a series of steps in different parts of the brain linked together into the emotion processing network. This network includes structures such as the prefrontal cortex, the cingulate cortex, the amygdala, the hippocampus, and the basal ganglia.
The neurons in these structures communicate through neurotransmitters like dopamine, serotonin, and norepinephrine, which are released from one neuron and bind to receptors of another neuron to modulate its activity. Dopamine is essential to modulate functions like learning, emotion, and reward mechanisms. Serotonin is involved in the regulation of mood, sleep, appetite, and libido. Finally, norepinephrine is involved in mood, focus, attention, and sleep.
Okay, so mood disorders are thought to be caused by neurotransmitter imbalances in the brain. Risk factors for mood disorders include genetic predisposition; personal or family history of a mood disorder; history of trauma or psychosocial stressors; substance misuse; age under 40; being assigned female at birth; and giving birth; among many others.
Now, the mechanisms underlying the pathology of mood disorders are poorly understood, but there seems to be abnormal neurotransmitter release or receptor availability. As a result, communication between neurons in the emotion processing network is impaired. Neurotransmitters can either be decreased, leading to reduced neuron activation and depression; or they can be increased, leading to excessive neuron activation and mania.
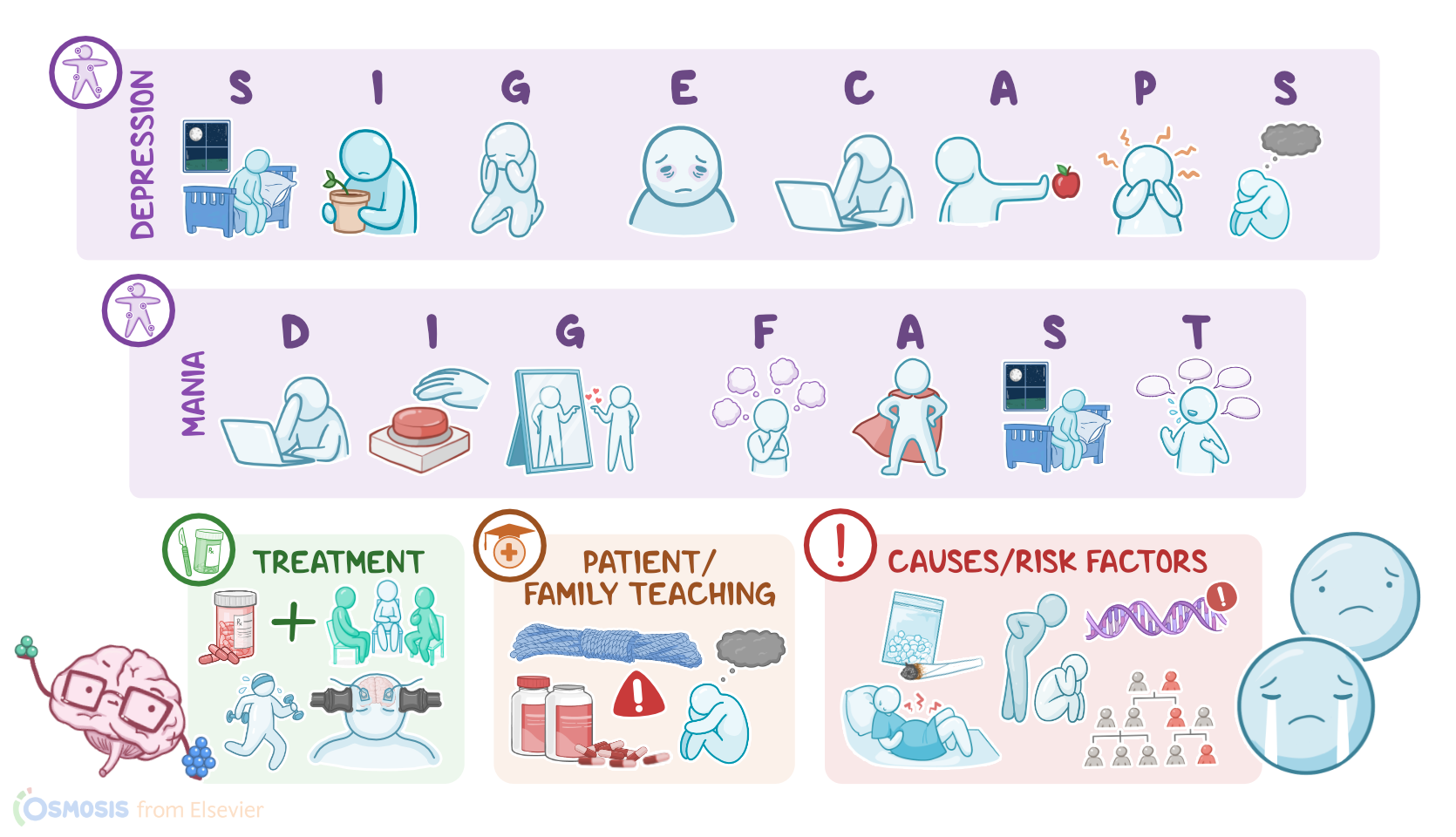
So mood disorders can have a spectrum of clinical manifestations that may cause significant impairment at school, work, or social life. On one end of the spectrum, there’s depression, where the main clinical manifestations can be summarized with the mnemonic SIG E CAPS. So, many clients experience Sleep disturbances, such as an increase in sleep during the day, or decreased sleep at night. Then there’s Interest loss, or anhedonia, which refers to a diminished interest in everyday activities that used to be pleasurable, like their hobbies.
Additionally, clients may experience Guilt or feel sad, hopeless, and worthless; as well as lack of Energy and feeling extremely fatigued. Some clients may also have Concentration difficulty, and slowing down of their thoughts or emotional reactions. Clients may also experience changes in Appetite; as well as Psychomotor agitation with anxiety, or lethargy. Finally, clients might have recurrent Suicidal thoughts or preoccupation with death.
On the other end of the spectrum, there’s mania, where the main clinical manifestations can be summarized with the mnemonic DIG FAST. So, many clients experience Distractibility and poor focus; as well as Irresponsibility and Impulsivity, showing reckless behavior, without any regard for later consequences. In addition, mania is characterized by Grandiosity, where clients might have a really high self-esteem or self-image.
Also, they might have Flight of ideas or racing thoughts; as well as increased Activity, since these clients may feel the need to engage in extreme goal-directed activities to achieve certain things. Clients with mania often have a Sleep deficit, or a severely decreased need for sleep, sometimes staying awake for days; and lastly, they often exhibit Talkativeness or pressured speech. On the same spectrum, some clients may experience a hypomanic episode, which is characterized by the same clinical manifestations, but they’re more mild than in a manic episode.
Diagnosis of mood disorders is based on detailed history and physical assessment. Particular attention should be given to the evaluation of suicidal thoughts. Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a mental health condition.
Now, based on the DSM-5 criteria, mood disorders can be categorized into two broad groups, which include depressive disorders and bipolar disorders. To diagnose a depressive disorder, the client must experience at least one depressive episode that lasts for at least two weeks and includes five depressive symptoms, one of which should be either depressed mood or anhedonia. Depressive disorders include major depressive disorder; major depressive disorder with seasonal pattern; major depressive disorder with psychotic features; major depressive disorder with peripartum onset; depression with atypical features, and persistent depressive disorder.
On the other hand, to diagnose a bipolar disorder, the client must present at least one manic or hypomanic episode, which tends to last for several weeks or months. Typically, these episodes fluctuate with depressive episodes, and in between, the client may even have periods of remission and stable mood.
Treatment of mood disorders usually involves a combination of psychotherapy and pharmacotherapy. Psychotherapy, including cognitive-behavioral therapy, focuses on teaching the client strategies to better cope with stress and social pressures, as well as to identify the patterns of thought that might be influencing their disorder. In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Regarding pharmacotherapy for depression, the first line antidepressant medications are selective serotonin reuptake inhibitors or SSRIs, such as fluoxetine, paroxetine, or sertraline. These should be titrated up according to response and be continued for at least 6 months post symptom resolution. Other antidepressant classes include serotonin and norepinephrine reuptake inhibitors or SNRIs like duloxetine, venlafaxine, or desvenlafaxine; atypical antidepressants like mirtazapine or bupropion; tricyclic antidepressants or TCAs like amitriptyline or nortriptyline; and monoamine oxidase inhibitors or MAOIs like isocarboxazid or selegiline.