Multiple sclerosis (MS): Nursing
2,066views
Notes
| MULTIPLE SCLEROSIS (MS) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Multiple sclerosis or MS is an autoimmune degenerative nerve disorder that causes demyelination of the nerve fibers of neurons in the brain and the spinal cord. This demyelination occurs when the body's own immune system inappropriately attacks and gradually destroys the myelin sheath, slowing down the communication between neurons.
Let’s start by looking at the physiology of neurons. Remember that neurons are the cells of the brain and spinal cord that transmit electrical signals throughout the central nervous system and the body. These signals are transmitted as nerve impulses, which move across a branch of the neuron called axon, which is covered by a protective myelin sheath. The role of this sheath is to speed up the transmission of electric impulses, allowing information to travel quickly from one neuron to another in order for us to perceive sensations and perform movements.
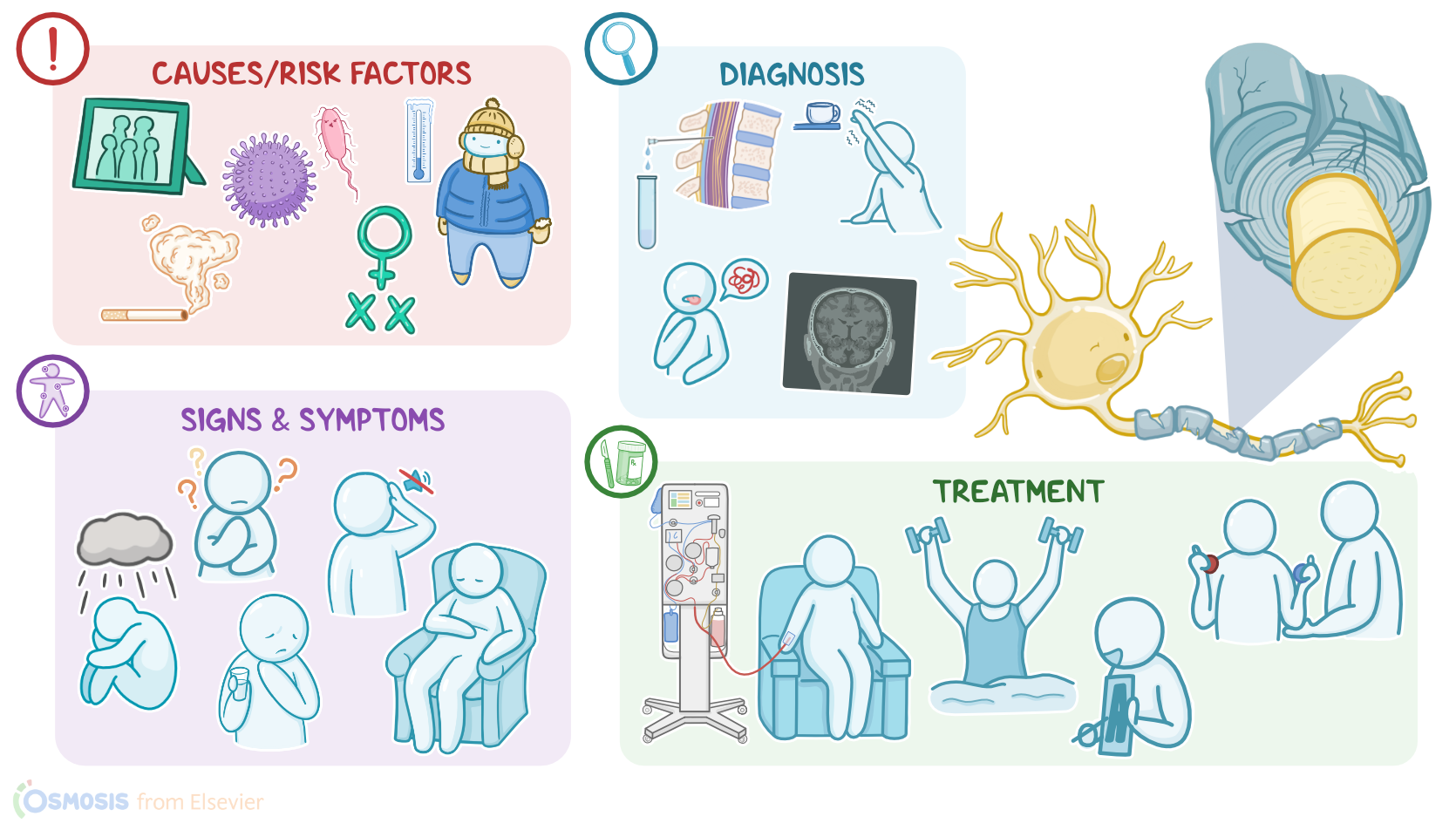
Just like other autoimmune diseases, the exact cause of MS is unknown, but it is linked to both genetic and environmental factors. Multiple sclerosis typically affects clients between the ages of 20 and 40, and genetic risk factors include a family history of MS, clients assigned female at birth, as well as genes that encode a specific type of immune molecule, called HLA-DR2, which is used to identify and bind to foreign molecules. Environmental risk factors might include infections, smoking, and living in a colder climate, as well as vitamin D deficiency. This is an interesting one, because it might help explain why the rates of multiple sclerosis are higher among the clients living at higher latitudes, compared to the clients living closer to the equator where there’s a lot more sunlight.
Together, these genetic and environmental factors trigger the activation of the body’s own immune cells that enter the CNS, target the myelin and cause widespread inflammation. As inflammation progresses, it gradually damages the axons as well. This impairs the transmission of nerve impulses leading to all sorts of sensory, motor, and cognitive problems. Now, when it comes to clinical manifestations, it’s worth noting that the onset of MS is very slow and gradual, so specific signs and symptoms vary a lot from clients to clients depending on the severity of the disease. One common trio of signs is called Charcot’s neurologic triad, including dysarthria, which is difficult or unclear speech; nystagmus, which is involuntary rapid eye movements; and an intention tremor. Other symptoms include double vision or blurred vision, hearing loss, short term memory loss, fatigue, generalized weakness, impaired swallowing, and loss of sensation and coordination, as well as impaired bowel and bladder function. Clients may also develop anxiety, and depression.
Now, based on the pattern of symptoms, MS is classified into four main types: relapsing-remitting, primary-progressive, secondary-progressive and progressive-relapsing. With relapsing-remitting MS, symptoms develop but resolve within a few weeks or months and the client returns to partial or complete remission. In primary-progressive MS, steady neurologic deterioration occurs without any remission. In secondary-progressive MS, a relapsing-remitting course later becomes a steady progression of symptoms. Finally, with progressive-relapsing MS, the disease continues to progress, and there are frequent relapses with only partial recovery, but no full return to normal.
Now, there are no definitive diagnostic tests available as of now for MS. Multiple sclerosis is typically suspected when clients give a history of multiple neurologic symptoms separated in space and time. The diagnosis of multiple sclerosis is supported by an MRI of the brain and spinal cord. In addition, a CSF analysis can be done, which might show high levels of antibodies, indicating an autoimmune process. Finally, a visual evoked potential, or VEP, can be helpful as well, measuring the nervous system’s response to visual stimuli.
Unfortunately, there is no cure for multiple sclerosis, but there are medications which are particularly effective in treating the relapsing-remitting type. Immunomodulators like corticosteroids, cyclophosphamides, a cell cycle inhibitor, and intravenous immunoglobulin can be used to help blunt the autoimmune process, as well as monoclonal antibodies, interferons or fumarates. In addition, plasmapheresis, when the plasma is filtered to remove disease-causing autoantibodies, can be effective. Chronic treatment for multiple sclerosis includes immunosuppressants. Physical therapy like water exercise, occupational therapy, speech therapy, deep brain stimulation and dorsal-column electrical stimulation can be utilized in improving the sensory, motor, and cognitive symptoms. Finally, new research on stem cell therapy has been going on to manage aggressive or treatment-resistant forms of MS.
All right, now let’s talk about nursing you'll provide for a client with a multiple sclerosis exacerbation. Your goals of care are to provide symptom relief, prevent complications, and provide emotional support. Begin providing symptom relief by assessing their current level of neuromuscular function. Then, institute fall precautions and administer the prescribed IV corticosteroids. Continue to monitor your client’s response to treatment, and report if symptoms such as extreme weakness, loss of balance, dysarthria, dysphagia, and loss of vision continue in spite of corticosteroids. As ordered, prepare your client for plasmapheresis.