Physical assessment - Musculoskeletal system: Nursing
Physical assessment - Musculoskeletal system: Nursing
IT?S MEGHAS LIST
IT?S MEGHAS LIST
Notes
| PHYSICAL ASSESSMENT - MUSCULOSKELETAL SYSTEM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| GETTING STARTED |
| |
| ANATOMICAL LANDMARKS |
| |
| METHODS OF ASSESSMENT |
| |
| INSPECTION |
| |
| PALPATION |
| |
| SPECIAL TESTS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Assessment of the musculoskeletal system should be completed as part of a comprehensive assessment, like during a routine physical exam, or as part of a focused exam if a client is experiencing musculoskeletal pain or has sustained an injury. Examination of the musculoskeletal system gives the nurse information about the mobility and stability necessary for physical movement. Let’s review the process of completing a musculoskeletal system assessment.
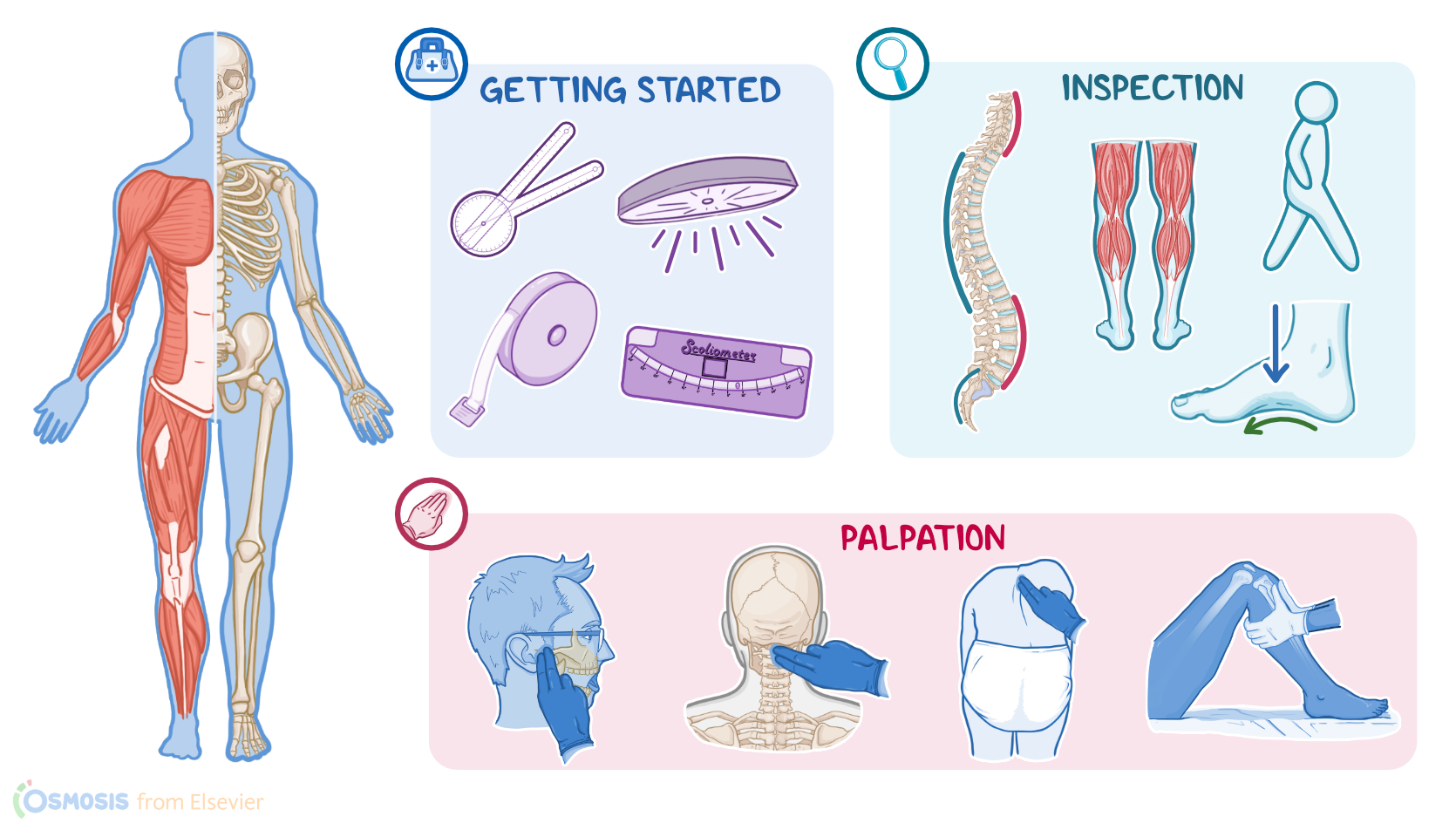
Okay, the supplies you’ll need for your assessment include a goniometer, scoliometer, a tape measure, and a good source of light. Prepare for the exam by ensuring your client is in a comfortable position, that your hands are warm, and that the temperature in the room is comfortable. Provide privacy by closing the door and curtains, properly draping your client, and only exposing areas of their body as needed to perform your examination.
Remember to position your client to ensure they’re safe and stable, and adapt positioning to address any current injury or complaints. Assess for a history of unilateral weakness, stroke, or mobility issues, and plan to have an assistant in the room if your client has joint instability or is at risk for falling. Before getting started, explain the procedure to your client and be sure to answer any questions they might have before obtaining verbal consent. Then, perform hand hygiene and collect your supplies.
Now, locating the anatomical landmarks of the musculoskeletal system will help guide the appropriate placement of your equipment and hands throughout your assessment. As you assess the various structures of the musculoskeletal system, you should move systematically, starting from the head and neck, and moving down to the feet and ankles, locating specific landmarks for each area. So, when you’re assessing the temporomandibular area, important landmarks include the tragus of each ear, whereas the landmarks of the hips are the iliac crests and greater trochanters.
The methods of assessment for the musculoskeletal system include inspection and palpation. There are also specialty tests for range of motion and muscle strength and tone.
Alright, so inspection of the musculoskeletal system begins when you first meet your client, as you assess their gait, posture, and signs of pain as they move into the examination room. Normally, clients should have an upright posture and ambulate with an even, smooth, painless gait. As your client is standing, inspect their general body shape and structure. Then, inspect the spine from the neck to the hips, and check for the normal curves of the spine, which include a concave curve of the cervical and lumbar spines, and a convex curve of the thoracic and sacral spines.
Note any alterations in spinal curvature such as lordosis, or an exaggerated inward curvature of the lumbar spine, sometimes seen in pregnant clients; kyphosis, where the top of the spine appears more rounded than normal, which can occur in elderly clients; and scoliosis, or a lateral curvature of the spine, usually discovered in childhood.
Also inspect the limbs, which should be bilaterally symmetric in length, circumference, alignment, and position. Next, inspect the muscles which should be symmetrical bilaterally. Unexpected findings include fasciculations, or muscle twitching, which can occur if the motor neuron supplying the muscle is damaged; or muscle wasting, which can occur after an injury, or due to a muscle disease.
Okay, starting with the head and neck, and viewing posteriorly, the head should be positioned in midline and aligned with the shoulders, spinal column, and gluteal cleft, which is the groove between the buttocks located just below the sacrum. The shoulders should be symmetrically positioned on either side of the upper trunk. Moving down, the iliac crests of each hip should be even and symmetrical. Then, check the knees, which should be aligned with the trunk. Note if they deviate outward, called genu varum or bow leg; or if they deviate inward, called genu varus, or knock knee.
Then, inspect the ankles, feet, and toes, which should face forward and align with the tibia bones. Also check where your client is bearing the weight of their body which, overall, should be on the midline of the foot. Deviations in foot alignment, heel pronation, pain, and injuries can all cause the position of weight bearing to be shifted. Each foot should have a longitudinal arch; however, over time, the feet can begin to flatten as a result of weight bearing. Other foot variations include pes planus, or a foot that stays flat even when not bearing weight, and pes cavus, which is a higher than normal instep.
Finally, inspect the toes, which should appear straight, flat, and pointing forward. Abnormalities of the toes include hammertoe, where the middle joint is bent; claw toe, where the toes are bent in a claw-like position; hallux valgus, or bunion, where there’s a lateral deviation of the hallux, or great toe; and hallux varus where the great toe deviates away from the other toes.
Next, palpate your client’s bones, joints, tendons, and muscles. Typically, the joints should be aligned, symmetrical, and nontender. There should be no crepitus, or a grating sensation, which can be present when a client has tendinitis or when the rough edges of a bone rub against each other; or edema, which can occur due to gout, arthritis, or injury.
Now, starting with the head, palpate the temporomandibular joint by placing your fingers in the joint space that appears anterior to the tragus of the ears, as your client opens and closes their mouth. If there’s a slight popping sound or sensation, this can be normal as long as there are no other symptoms like pain. Moving onto the cervical spine, palpate down the posterior neck and surrounding muscles.