Physical assessment - Neurological system: Nursing
Physical assessment - Neurological system: Nursing
Clinical Nursing Skills & Technique
Clinical Nursing Skills & Technique
Notes
| PHYSICAL ASSESSMENT - NEUROLOGICAL SYSTEM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| GETTING STARTED |
| |
| ANATOMICAL LANDMARKS |
| |
| METHODS OF ASSESSMENT |
| |
| CEREBELLAR FUNCTION |
| |
| SENSORY FUNCTION |
| |
| MOTOR FUNCTION |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Assessment of the neurological system should be completed as part of a comprehensive client assessment, or as part of a focused exam if the client is experiencing issues that might be related to neurological function, like a facial droop or confusion. Now, let’s review the process of completing a neurological assessment.
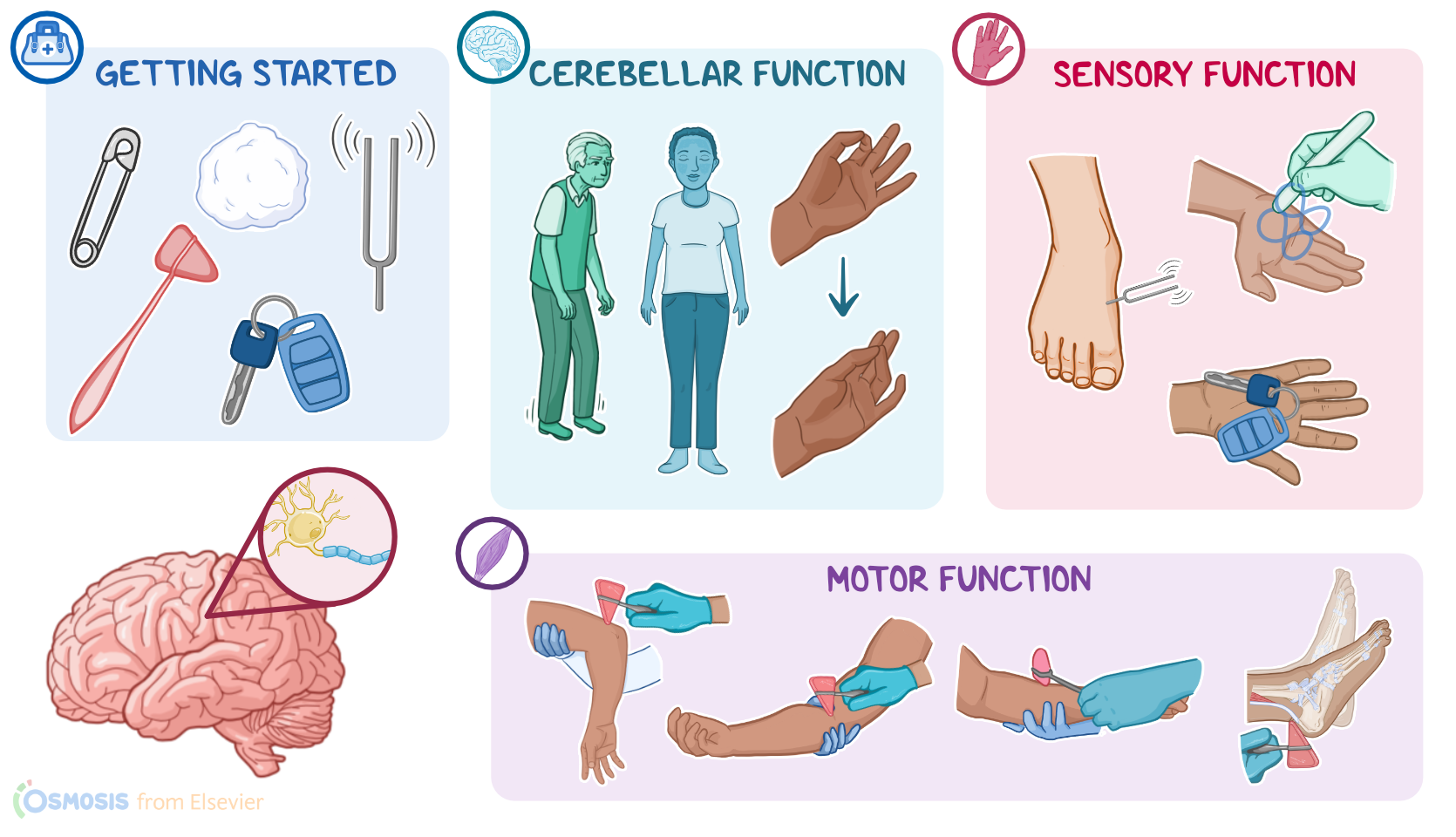
Okay, the supplies you’ll need include a cotton ball; a tuning fork; an object that can be easily recognized by touch like a paper clip, key, or coin; a reflex hammer; a tongue blade; drapes, and gloves.
Then, prepare for the exam by ensuring your client is in a comfortable position, that your hands are warm, and that the temperature in the room is comfortable. Provide privacy by closing the door and curtains, properly draping your client, and only exposing areas of their body as needed to perform your examination.
Before getting started, explain the procedure to your client and be sure to answer any questions they might have before obtaining verbal consent. Then, perform hand hygiene and collect your supplies.
While much of the neurological system assessment involves observation, you will need to locate the deep tendon reflexes to assess spinal cord intactness. Commonly tested deep tendon reflexes include the triceps, biceps, brachioradialis, patellar reflexes, and achilles reflexes.
Alright, the methods of assessment for the neurological system include inspection and palpation. Your assessment will evaluate your client’s cerebellar function, which includes the client’s balance and coordination; sensory function, which includes their ability to feel and differentiate between light touch and pain; and motor function, which includes deep tendon reflexes.
Okay, begin your assessment of cerebellar function by observing your client’s gait, or how they walk. You can take the opportunity to do this as they enter the examination room or, if they are seated or in a bed, you can ask them to stand and walk across the room. While they ambulate, take note of their posture, coordination, and the movement of their legs and feet. Their gait should appear smooth and steady without hesitation, shuffling, or swaying.
Next, test balance and equilibrium with the Romberg test. Ask your client to stand with their feet together with their eyes open, and their arms at their sides. They should remain balanced and their body shouldn’t sway. Next, ask them to close their eyes for about 30 seconds while you observe their ability to stay upright. Be sure to stay close to your client to support them in the event they lose their balance. Your client should be able to maintain their balance with only mild swaying. The Romberg test is abnormal if your client demonstrates a loss of balance, by excessive swaying, moving their feet, or if they begin to fall.
Finally, assess your client’s coordination by testing rapid alternating movements. This is done by asking them to tap the tip of their thumbs to the tip of each finger on their hands as quickly as possible. You should expect swift movement while making contact between the thumb and each finger. You can also perform this test by asking them to pat their thighs with both hands and then flip their hands, so they are alternating the palmar and anterior aspects of the hands. Your client should be able to make smooth contact with the surface of their thighs with increasing speed without pausing or faltering. Slow, uncoordinated, or jerky movements is called dysdiadochokinesis, and is an unexpected finding.
Okay, moving on to sensory function. Begin by testing your client’s ability to detect superficial touch. To do this, ask your client to close their eyes, and use a cotton wisp to gently touch the surface of the skin, on their face, arms, or legs. Expect them to tell you when and where they feel the cotton touch their skin.
Next, evaluate pain perception. Using the sharp and dull edges of a broken tongue depressor, and using the same technique as you did to test superficial touch, gently touch the pointed edge and dull edge to the skin, alternating between the two sides. Expect them to correctly identify the location and type sensation.
Now, to test for vibratory sensation, instruct your client to close their eyes, and place the stem of a vibrating tuning fork on a bony prominence, like the great toe joint. Expect them to tell you when they feel the vibration and when it stops.