Physical assessment - Thorax and lungs: Nursing
Notes
| PHYSICAL ASSESSMENT - THORAX AND LUNGS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| GETTING STARTED |
| |
| ANATOMICAL LANDMARKS |
| |
| METHODS OF ASSESSMENT |
| |
| INSPECTION |
| |
| PALPATION |
| |
| PERCUSSION |
| |
| AUSCULTATION |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Assessment of the thorax and lungs should be completed as part of a comprehensive assessment, like during a routine physical exam, or as part of a focused exam if a client is experiencing respiratory issues like shortness of breath, cough, or chest discomfort. Examination of the thorax and lungs gives the nurse information about the movement of air and gas exchange. Let’s review the process of completing thorax and lung assessment.
Okay, the supplies you’ll need for your assessment include a stethoscope, a washable pen or marker, a centimeter ruler, tape, drapes, and a good source of light.
Then, prepare for the exam by ensuring your client is in a comfortable position, that your hands and stethoscope are warm, and that the temperature in the room is comfortable. Provide privacy by closing the door and curtains, properly draping your client, and only exposing areas of their body as needed to perform your examination. Before getting started, explain the procedure to your client and be sure to answer any questions they might have before obtaining verbal consent. Then, perform hand hygiene and collect your supplies.
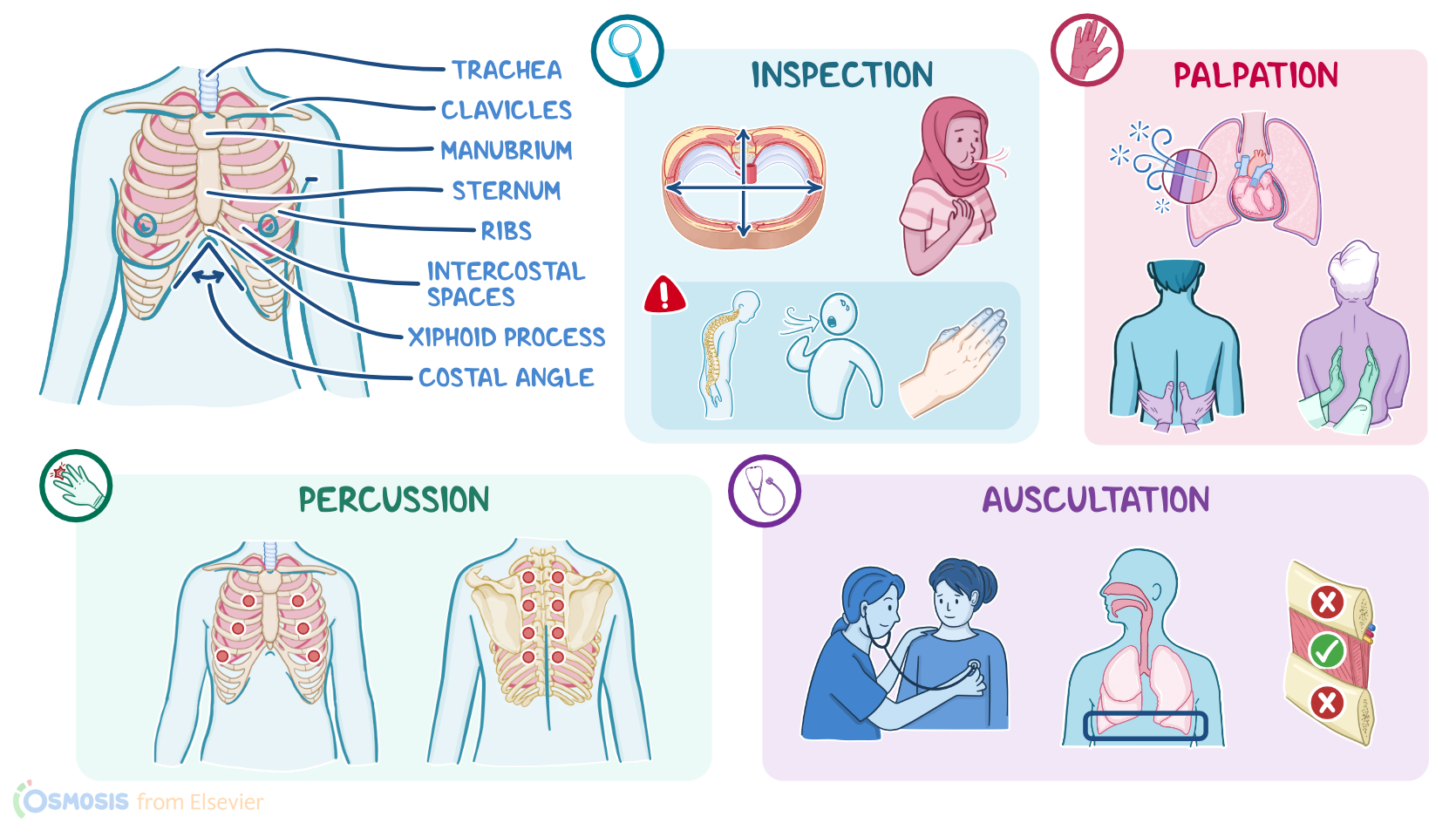
Now, locating the anatomical landmarks of the thorax and chest will help guide the appropriate placement of your equipment and hands throughout your assessment. The thorax can be divided into the anterior chest and posterior chest. Commonly used anterior landmarks include the sternum, clavicles, manubrium, xiphoid process, the ribs and intercostal spaces, and trachea, as well as the costal angle, which is made up of the the costal margins just below the xiphoid process. The chest can be further divided into sections using the midsternal line, a vertical line that runs down the middle of the sternum; and the right and left midclavicular lines, which are parallel to the midsternal line and run from the middle of each clavicle to around the 6th intercostal space. Posteriorly, the landmarks include the scapulae and thoracic spine. These lines are parallel to the spine and travel through the middle of the scapulae.
Now, methods of assessment for the thorax and lungs include inspection, palpation, percussion, and auscultation.
Okay, as you begin your assessment, be sure to watch your client closely for indications of respiratory discomfort. These may include facial expressions or other cues, such as a fast respiratory rate. Then, visualize the symmetry and shape of the chest both anteriorly and posteriorly. The anterior-posterior diameter of the chest should be less than the lateral diameter. When these are equal, it is referred to as barrel chest. With a barrel chest, you may also notice the slope of the ribs will be more parallel, rather than the normal slightly downward slope, and the costal angle will be more than 90 degrees. A barrel chest can indicate a chronic respiratory condition, such as chronic obstructive pulmonary disease, or COPD for short, or cystic fibrosis.
You should also inspect the chest, spine, rib cage, sternum, and trachea for structural abnormalities, such as pectus carinatum, also known as pigeon chest, where the sternum bulges outward, and pectus excavatum, or funnel chest, where the sternum is depressed inward. Other structural abnormalities include scoliosis, where there’s an abnormal sideways curve of the thoracic and lumbar spine; and kyphosis, or an exaggerated outward curvature of the thoracic spine. Lastly, a deviation of the trachea can be related to thyroid disease, a mediastinal tumor, or pleural effusion.
Also observe your client’s respirations, which should be between 12 to 20 breaths per minute. A respiratory rate over 20 breaths per minute is considered tachypnea and may occur due to anxiety, pain, or infection, whereas a respiratory rate of less than 12 breaths per minute is considered bradypnea and may occur because of an electrolyte imbalance or the effects of opioid medications.
In addition to the respiratory rate, note your client’s respiratory pattern, which should be regular and unlabored. Be sure to assess for signs of acute respiratory distress, including retractions, which occur as a result of airway obstruction, causing the chest wall to “pull in'' at the sternum and between the ribs as the muscles try to overcome the obstruction; and nasal flaring, which occurs when the nostrils widen during inhalation in an attempt to take in as much oxygen as possible. Clubbing of the fingers is a sign of chronic respiratory disease. Also check your client for cyanosis, or the bluish discoloration of the skin, mucous membranes, and nail beds, that is a late sign of hypoxia.
When assessing for color changes, remember to always consider the natural variations in skin tone. For example, cyanosis in a client with light skin, will appear as blue or purplish coloring. On the other hand, in clients with darker skin, cyanosis can appear as a grayish or whitish discoloration which can be more easily seen in the mucous membranes, lips, conjunctiva, and nail beds. In clients with a more olive complexion, cyanosis can take on a gray or greenish hue.