Poliomyelitis: Nursing
Introduction0:00–0:22
0:04
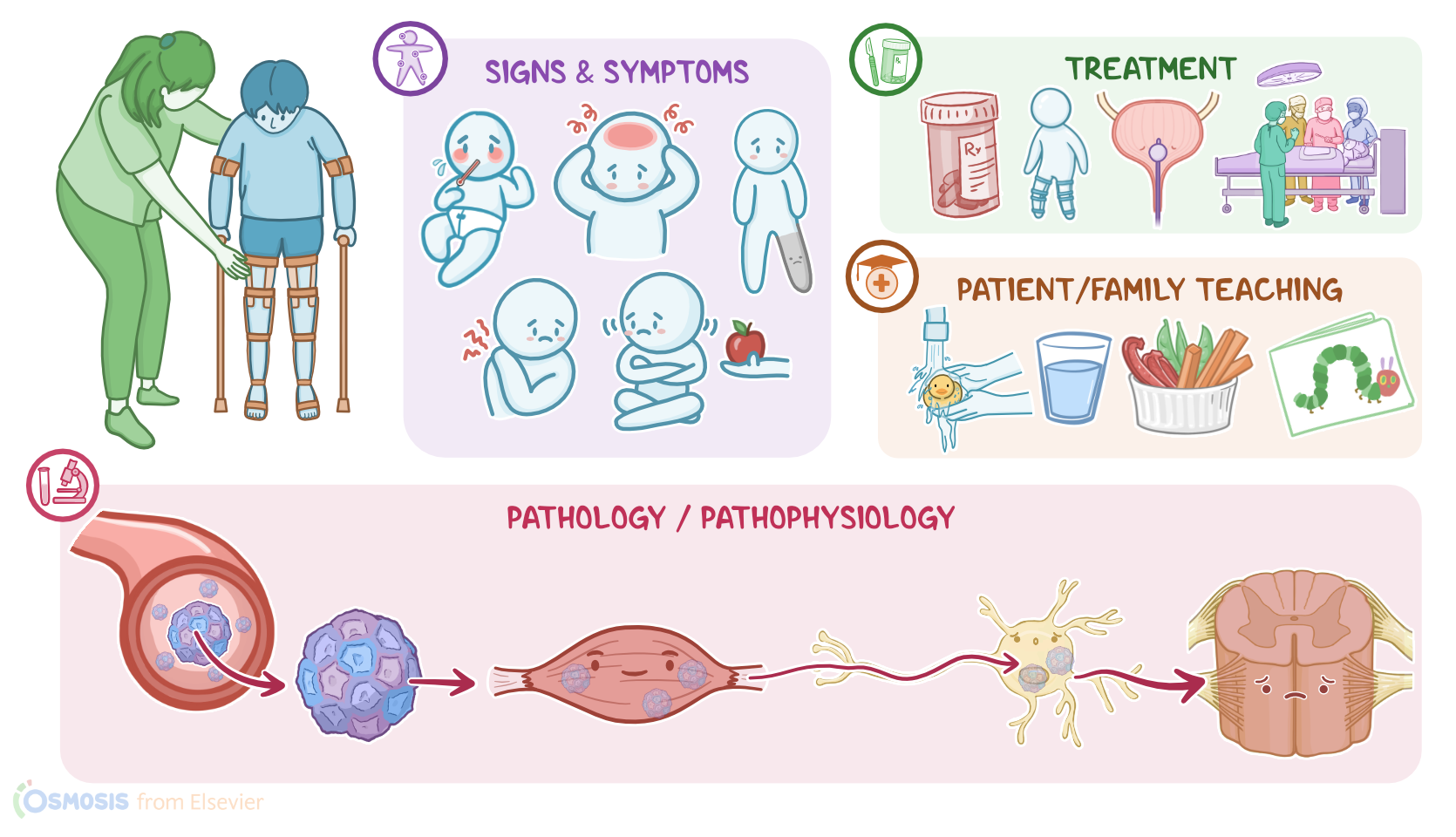
Poliomyelitis is a highly contagious viral infection that leads to severe nerve injury. It is caused by the poliovirus, which moves from the gut to the central nervous system.
0:16
This can cause irreversible paralysis, breathing difficulties, and even death. Let’s start with a quick review of the physiology of the upper gastrointestinal system, which consists of the mouth, pharynx, esophagus, stomach, and the first part of the small intestine, called the duodenum.
Physiology0:22–1:27
0:32
Now, let’s zoom into the wall of the gastrointestinal tract, which is made up of four layers. The outermost layer is called serosa or adventitia.
0:44
0:54
And finally, there’s the innermost layer, called the mucosa, which consists of a layer of epithelium covering the lamina propria.
1:03
The epithelium acts as a physical barrier that prevents harmful pathogens from entering the body. Additionally, the lamina propria houses immune cells, like dendritic cells and macrophages, that react to harmful pathogens.
1:18
Additionally, round accumulations of lymphatic cells, called Peyer’s patches, can sometimes be found in the mucosa of the duodenum.Now, the main cause of poliomyelitis is the poliovirus, which is an RNA virus that belongs to the Enterovirus genus, and the Picornaviridae family.
Causes & risk factors1:27–1:52
1:37
Important risk factors for poliomyelitis include immunodeficiency; age below 5, being unvaccinated or undervaccinated; and finally, living in poor sanitary conditions, or traveling to an endemic area.
1:50
Alright, now the pathology of poliomyelitis starts with acquiring the virus through the fecal-oral route through contaminated water or food.
Pathology1:52–3:49
2:00
In some cases, it could also be transmitted through droplets produced by a sneeze or cough. Once in the gastrointestinal tract, the virus binds to receptors on the membrane of epithelial cells in the upper gastrointestinal tract and enters the cell.
2:15
Inside the cell, the virus creates new viral particles and creates new viral particles and starts to replicate. Within days, these cause the epithelial cell to lyse, meaning the cell breaks down, releasing the newly formed viruses, which then make their way to nearby lymph nodes and eventually into the bloodstream.
2:38
Poliovirus prefers to infect motor nerves, so oftentimes it will leave a blood vessel and get into the interstitial tissue of muscle tissue.
2:46
From there, poliovirus invades the motor neuron and travels retrograde to the anterior horn of the spinal cord, which houses lower motor neurons.
2:49
Infected motor neurons attract immune cells like neutrophils and macrophages which cause inflammation and damage to the spinal cord.
2:59
As infected motor neurons die, the muscles of the trunk and limbs no longer receive signals from the brain or trophic factors which causes the muscles to start to atrophy and become weak.When it comes to complications of poliomyelitis, these include paralysis with bulbar involvement.
3:17
This occurs when the poliovirus affects a part of the brainstem that houses cranial nerves involved in speaking and swallowing.
3:24
This part of the brain stem also regulates breathing and heart rate, so it can lead to blood pressure fluctuation, or fatal respiratory and cardiovascular collapse.
3:33
Finally, some clients develop post-polio syndrome or PPS for short, which is characterized by new-onset or progressive muscle weakness that can show up in polio survivors years or decades after the initial infection.
3:47
Clients with poliomyelitis initially present with flu-like symptoms, including fever, malaise, headache, anorexia, and sore throat.
Clinical manifestations3:49–4:18
3:56
Other signs and symptoms include abdominal pain, as well as soreness and stiffness of the neck, trunk, and limbs, and eventually loss of muscle reflexes, and acute flaccid paralysis.
4:07
Usually the paralysis develops over a few days and is asymmetric; most often affecting larger proximal muscles, especially in the thighs.
4:16
The diagnosis of poliomyelitis starts with the client’s history and physical assessment, followed by detection of poliovirus-specific IgM and IgG antibodies.
Diagnosis4:18–4:56
4:30
Additionally, a reverse transcription polymerase chain reaction, or RT PCR, can be used to detect viral RNA in the stool, throat, blood, or cerebrospinal fluid.
4:41
Also, samples of these bodily fluids can be used to prepare viral cultures and look for infected cells. Finally, imaging tests, like an MRI of the spinal cord, might be performed to assess the extent of the disease.There’s no specific treatment for polio, but the key is supportive care.
Treatment4:56–6:24
5:02
Typically this includes pain medication to help with muscle spasms. Clients might also need respiratory support if they have trouble breathing.
5:10
Bladder weakness or paralysis can be managed by placing a urinary catheter. Surgical management can also be done to prevent deformities and regain mobility.
5:21
Lastly, rehabilitation is provided to maintain range of motion, improve strength, and prevent limb deformities and contractures.
5:30
Fortunately, it’s possible to prevent infection with a vaccine. The polio vaccine comes in two forms; inactivated polio vaccine, or IPV, which is the only form of vaccine available in the US, in addition to live-attenuated oral polio vaccine, or OPV for short.
5:46
Now, for clients who were exposed to the virus, certain measures should be taken to minimize the risk of infection. These include washing the area of the skin exposed to the virus with water and soap for at least 15 minutes.
6:00
Additionally, the exposed area should be decontaminated with antiseptic scrub solution. When the mucous membrane of the eyes, nose, or mouth are exposed to the virus, these should be vigorously irrigated.
6:14
Garments exposed to the virus should also be removed and placed in a double red plastic bag to avoid further exposure. Okay, let’s talk about the nursing care you would provide for a pediatric client with poliomyelitis.
Management and care6:24–8:23
6:29
Your primary nursing goals are to prevent spread of the virus to others, monitor for complications, and provide supportive care.Begin by instituting standard and contact precautions and maintaining bed rest.
6:43
Assist your client into a position of comfort while maintaining proper body alignment to help prevent contractures. Assess their level of pain and anxiety, and administer the prescribed analgesics, anxiolytics, and antipyretics as needed.Next, monitor their vital signs and encourage them to cough and deep breathe to help prevent pneumonia.
7:08
Watch them closely for signs of impending respiratory paralysis, and immediately report if they have an ineffective cough, difficulty talking, or if they have a rapid or shallow respiratory rate.
7:18
Support them by positioning them into a high Fowler position, provide high-flow oxygen through a non-rebreather mask, and prepare for further measures to support respiration, such as mechanical ventilation.Also be sure to address your client’s neuromuscular problems.
7:35
Provide support for their mobility limitations by assisting with repositioning and checking for skin breakdown. Apply moist warm packs to the affected limbs to ease muscle spasms, and help them with range of motion exercises.
7:51
Collaborate with the physical therapist to plan a rehabilitation program for your client, and the application of orthopedic devices to promote mobility and to prevent deformities.
8:01
Also keep a close eye on your client's bowel and bladder function. Report to the healthcare provider right away if your client experiences constipation and urinary retention.
8:11
Insert a urinary catheter to drain the bladder, as ordered; and assist with interventions to support elimination. Finally, ensure the case has been reported to the local health department.Okay, moving onto client and family teaching.
General client and family teaching8:23–10:07
8:27
Start by explaining that poliomyelitis is a highly contagious viral infection that leads to severe injury to the nerves, resulting in muscle weakness and paralysis.
8:38
Let them know that it is easily spread person-to-person mostly through the fecal-oral route, and sometimes through respiratory droplets.Teach them how they can avoid spreading the virus by reviewing infection control techniques such as frequent hand hygiene, helping their child to cover their mouth and nose with a tissue when coughing or sneezing, avoiding sharing utensils and cups, and washing the child’s toys.
9:05
Also remind them to avoid touching their eyes, nose, and mouth. Lastly, stress the importance of being fully vaccinated against polio.
9:11
While their child recovers, teach them to offer plenty of fluids and provide healthy snacks. Instruct them to encourage their child to rest and engage in quiet activities like reading or coloring.
9:28
Teach them that ibuprofen or acetaminophen can be given to help decrease pain and fever, and emphasize the importance of avoiding aspirin to prevent Reye syndrome, which can cause liver and brain damage.Also be sure to reinforce the use of assistive and orthopedic devices.
9:46
Remind them to participate actively in their child’s rehabilitation and follow-up with their healthcare provider for continued monitoring and support.Finally, instruct them to notify their healthcare provider immediately if their child experiences any new symptoms like trouble breathing or swallowing, excessive fatigue, or progressive weakness.Alright, as a quick recap… Polio is a highly contagious viral illness that is spread through fecal-oral or droplet transmission.
Review10:07–11:36
10:13
Polio can be prevented with the inactivated polio vaccine, or IPV, or the live-attenuated oral polio vaccine, or OPV for short.
10:24
Those that are most at risk for acquiring the illness are unvaccinated infants and young children under the age of 5, those living in areas with poor hygiene, those who have recently traveled to endemic areas, and those who are unvaccinated.
10:38
Symptoms include flu-like symptoms such as fever, malaise, headache, sore throat and mild respiratory tract infection. They may also have progressive soreness and stiffness in their trunk, limbs, and neck that becomes acute flaccid paralysis.
10:59
Diagnosis is based on history and physical assessment, as well as through detection of poliovirus-specific IgM and IgG antibodies, through RT PCR to identify viral RNA in body fluids, or through viral cultures.
11:11
Treatment of polio includes supportive treatment of the client’s symptoms. Goals of nursing care include preventing the spread of the virus to others, monitoring for complications, and providing supportive care.
11:29
Client and family education centers around infection control, providing care at home, and when to contact the healthcare
| POLIOMYELITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below