Postterm infant: Nursing
Notes
| POSTTERM INFANT | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
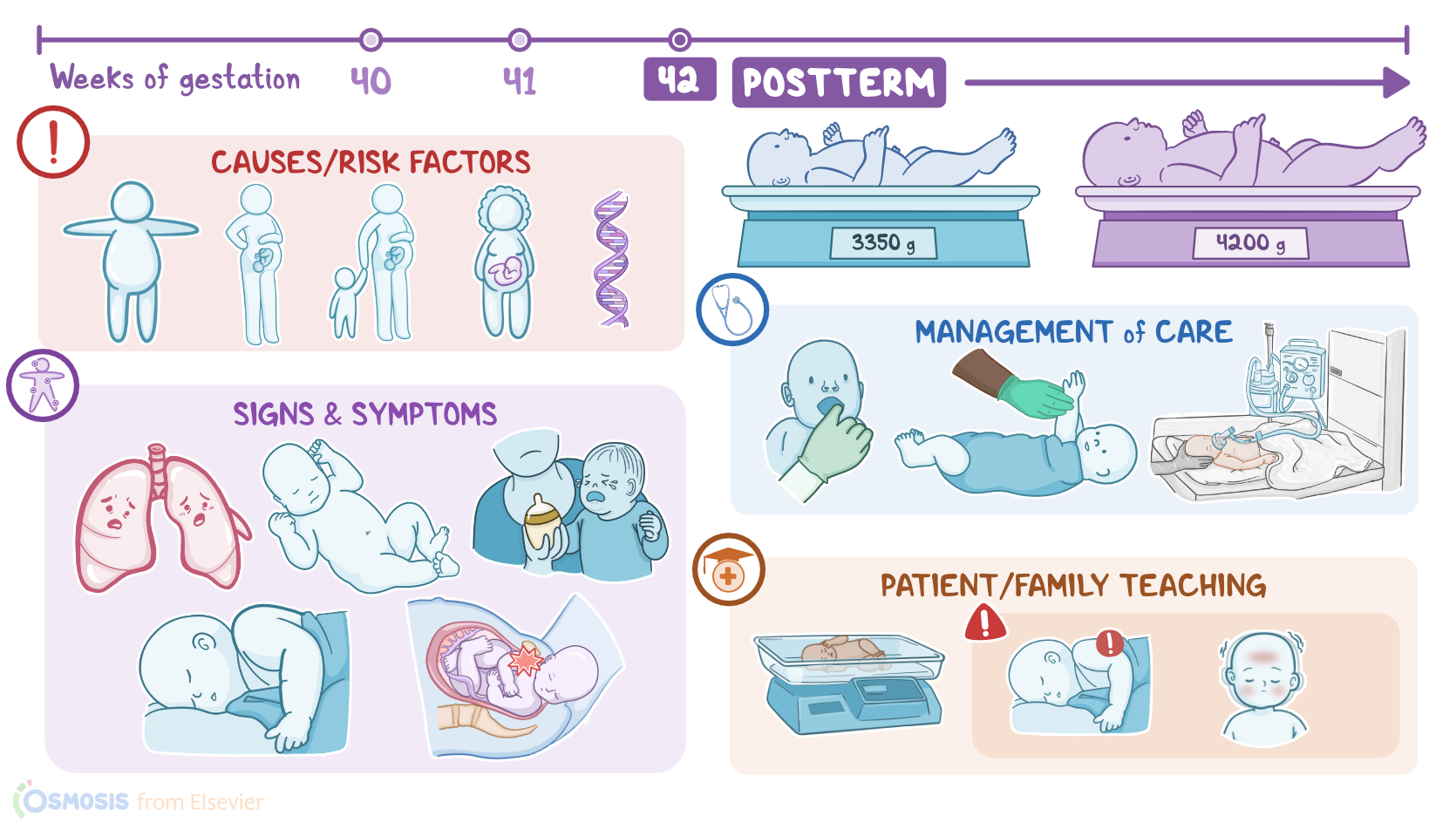
A postterm infant is any infant born after 42 weeks of gestation. A postterm infant could be small for gestational age or SGA; appropriate for gestational age or AGA; or large for gestational age or LGA. A postterm infant can also be dysmature, which means they have experienced wasting of subcutaneous fat and muscle. Let’s start with some basic physiology. Gestation refers to the period between conception and birth, which typically lasts for 40 weeks. During these 40 weeks, the embryo, and later fetus, grows and develops within the uterus. Normally, an infant comes to the world after 40 weeks of gestation, but every infant born between the 37th and 42nd week is considered a term infant. An infant born after the 42nd week is called a post-term infant.
Now, based on the gestational age and the infant’s birth weight, we can determine birth weight percentiles. Furthermore, birth weight percentiles help us evaluate the infant’s intrauterine growth and development, which is considered normal when the value is between the 10th and 90th percentile. For example, an infant born after 40 weeks of gestation that weighs around 3350 grams is within the 40th percentile. In other words, this baby is appropriate for gestational age, or AGA. On the other hand, an infant born after 40 weeks of gestation that weighs around 2400 grams is below the 10th percentile, and therefore small for gestational age, or SGA. Finally, an infant born after 40 weeks of gestation that weighs around 4200 grams is on the 95th percentile and is considered large for gestational age, or LGA.
Now, most commonly, the cause of postterm birth is unknown. The most important risk factors for postterm birth include obesity; first pregnancy or previous postterm pregnancies; and advanced maternal age. Genetic factors also influence postterm birth. Switching gears and moving on to pathology. The fetus will continue to receive a normal supply of oxygen and nutrients and growth will continue unchecked, as long as the placenta continues to function well. But, the longer the fetus stays within the uterus, the bigger it will get, so after birth, the infant often presents as LGA. On the flip side, if placental function deteriorates, the fetus won’t receive the oxygen and nutrients it needs. As a result, intrauterine malnutrition can occur, resulting in fetal dysmaturity, which occurs as the fetus uses up stored fat and muscle. So in this case, after birth, the infant often presents as SGA.
Now, decreased placental function can also cause the fetus to redistribute blood from less important organs, such as kidneys, to vital organs, like the brain. Less blood flowing to the kidneys results in less fetal urine production, which is the main component of the amniotic fluid during the second and third trimesters. Ultimately, this results in oligohydramnios, which is a condition when there is not enough amniotic fluid surrounding the fetus. This increases the risk of compression of the umbilical cord, further decreasing the supply of oxygen and nutrients to the fetus. Other fetal complications can include short-term and long-term complications. Short-term complications include hypoglycemia, polycythemia, and perinatal asphyxia. They are also at increased risk of meconium aspiration, which occurs when meconium, which is fecal material produced by the fetus during gestation, is passed into the amniotic fluid and enters the fetal respiratory tract.
Additionally, postterm infants can develop complications associated with macrosomia, like birth injuries such as fractures, subdural hematoma, and cephalhematoma, which refers to the accumulation of blood between the periosteum and the skull. In severe cases, fetal or neonatal death may occur. On the other hand, long-term complications can include cerebral palsy, seizures, as well as cognitive and developmental problems. Maternal complications, in case of vaginal delivery, usually include traumatic injuries of the perineal area, like lacerations, due to the passage of a physically large fetus through the birth canal. A large fetus also increases the risk of shoulder dystocia, where the fetal shoulders can’t progress past the maternal pubic bone after the fetal head has been delivered. Moreover, prolonged pregnancies increase the risk of cesarean delivery, which is associated with complications such as bleeding and infection.
Okay, in terms of clinical manifestations, large for gestational age infants are typically lethargic, obese, have a plethoric, or ruddy appearance, and often feed poorly. The infant could be jittery due to hypoglycemia; there are often signs of respiratory distress like tachypnea, and birth injuries could also be present. On the other hand, a dysmature infant is thin and SGA due to wasting of muscles and subcutaneous tissue. Their skin is dry, wrinkled, loose and they have very little to none vernix caseosa, which is a white, creamy, naturally occurring biofilm that covers the fetal skin. Also, these infants have no lanugo, but they do have profuse scalp hair and long nails, which can have a yellow to green color if exposed to meconium. Finally, they may have a thin umbilical cord with little Wharton’s jelly, which is a gelatinous substance that surrounds the umbilical blood vessels and protects them during the pregnancy.