Posttraumatic stress disorder (PTSD): Nursing
Posttraumatic stress disorder (PTSD): Nursing
NRS 428 WK 10 Other
NRS 428 WK 10 Other
Notes
| POSTTRAUMATIC STRESS DISORDER (PTSD) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
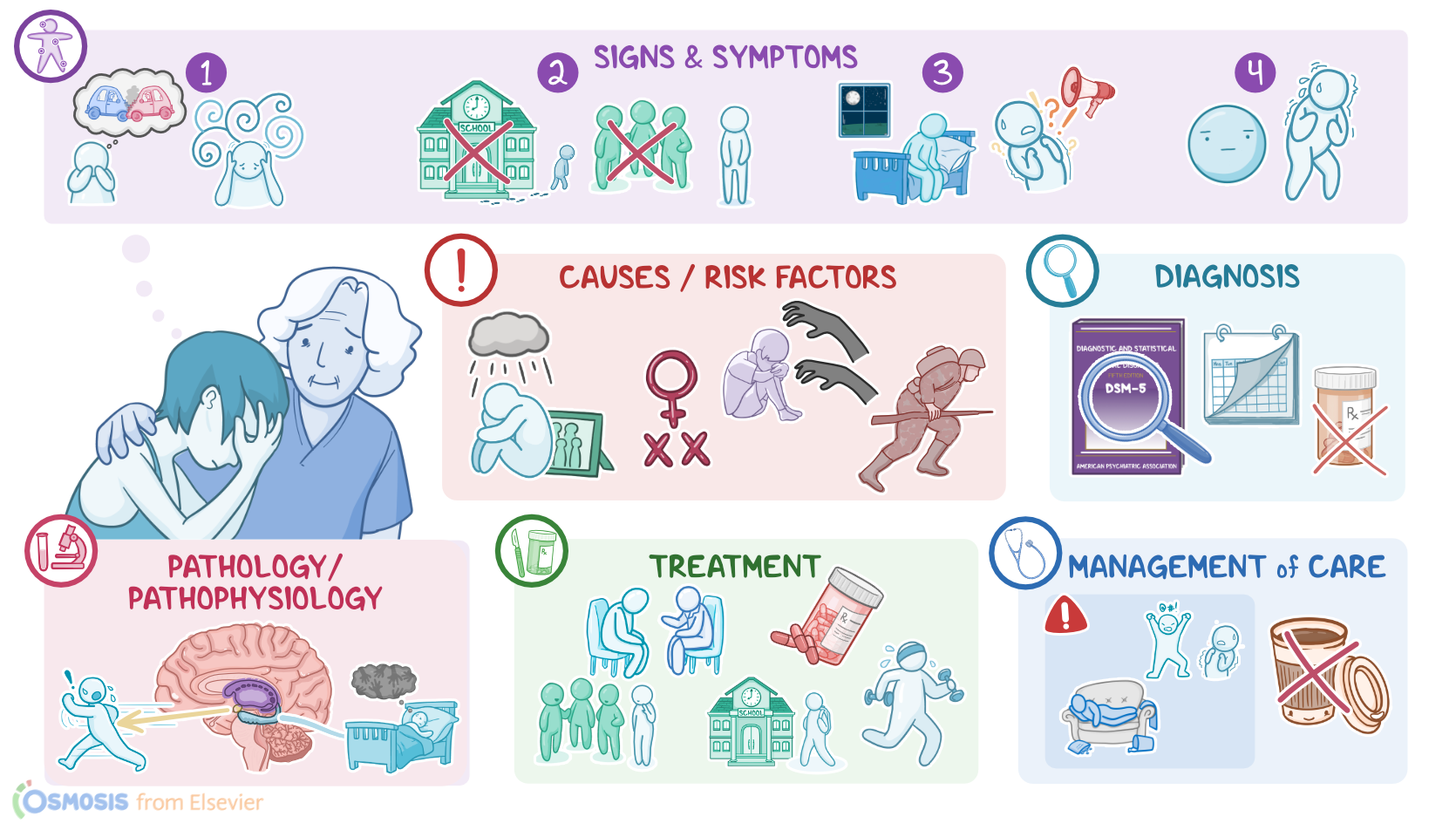
Posttraumatic stress disorder, or PTSD for short, is a mental health condition that occurs when a memory of a past traumatic event causes recurrent mental and physical distress. This condition usually occurs in clients who have either witnessed or directly experienced a traumatic event, like war or sexual assault.
Now, let’s focus on the physiology of the limbic system, which consists of a group of brain structures located under the cerebral cortex, including the amygdala, and hippocampus. Together these structures help regulate emotions, like anger and fear; as well as behavior, such as aggression and sexual activity.
The limbic system also influences memory formation and recollection of memories, especially those that contain a fear element; and it can even affect the response of the autonomic nervous system, like cardiovascular or gastrointestinal functions.
Additionally, the limbic system helps activate the fight or flight response, which occurs when a person is faced with a potential threat or stressful situation. The neurotransmitter involved in the regulation of the autonomic nervous system and fight or flight response is norepinephrine, which increases the heart rate, blood pressure, arousal, as well as startle response.
Now, the main cause of posttraumatic stress disorder is experiencing or witnessing a traumatic event, such as a life-threatening situation, physical injury, combat trauma, sexual assault, or child abuse.
Even though most people don’t develop posttraumatic stress disorder in response to a stressful event, some factors that increase the risk of this condition include personal or family history of mental health conditions, such as anxiety or depression; being assigned female at birth; military experience; childhood trauma; and finally, lower level of education.
Now, the mechanisms underlying the pathology of posttraumatic stress disorder are poorly understood, but there seems to be abnormal neurotransmitter release. As a result, communication between neurons in the limbic system is impaired. Some parts of the limbic system, like the amygdala, which triggers a fight or flight response, can become overactive, leading to fight or flight responses in the absence of an actual threat or danger. At the same time, other parts of the limbic system, like the hippocampus, which is responsible for memory formation, may become hypoactive, leading to recurrent memories about the event and flashbacks.
Alright, switching gears and moving on to clinical manifestations, which can be subdivided into four main groups. The first group covers intrusion symptoms, such as re-experiencing a trauma through intrusive thoughts, flashbacks, or nightmares. When exposed to reminders of their trauma, clients usually feel intense psychological distress or physical reactions, such as sweating, tachycardia, and palpitations.
The second group includes avoidant behavior, more specifically, avoidance of places, people, and situations that remind a client of their traumatic experience.
Next up are changes in arousal and reactivity, such as sleeping problems; hyperarousal, which refers to an exaggerated startle response to the smallest triggers, such as loud or sudden noises; and hypervigilance, which is a state of being constantly tense and on guard for potential threats.
Finally, the last group covers negative thoughts and beliefs about oneself, others, and the world. For example, a client might think that no one can be trusted or they might have persistent negative emotions, like feeling hopeless, detached, or emotionally numb.
Diagnosis of posttraumatic stress disorder is based on a detailed history and physical assessment. The diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a mental health condition. Now, based on the DSM-5 criteria, posttraumatic stress disorder is diagnosed in clients who were exposed to a traumatic event and whose symptoms persist for over a month. It’s important to note that these symptoms cannot be associated with medications, substances, or alcohol, or some other medical condition.
Treatment of posttraumatic stress disorder usually involves a combination of psychotherapy, and pharmacotherapy. Psychotherapy includes cognitive-behavioral therapy, or CBT, which focuses on teaching the client strategies to challenge negative thoughts, feelings, and behavior patterns; and exposure therapy, which slowly exposes a person to situations, people, and places that trigger psychological and physical distress. In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Regarding pharmacotherapy for posttraumatic stress disorder, the first line antidepressant medications are selective serotonin reuptake inhibitors or SSRIs, such as fluoxetine, paroxetine, or sertraline, and serotonin and norepinephrine reuptake inhibitors or SNRIs like duloxetine, venlafaxine, or desvenlafaxine. If these medications fail to alleviate symptoms of posttraumatic stress disorder drugs or monoamine oxidase inhibitors should be used. But, if a client fails to respond to second-line medications, they should be given antipsychotics. Finally, prazosin, which is an alpha-1 blocker, can be used to treat nightmares.
Let’s look at the care you will provide to a client with PTSD. Your priority goals are to improve psychological functioning and promote safety.
Begin by assessing your client’s anxiety level, including vital signs, mood, affect, and behavior. Establish a therapeutic relationship by providing a calm, quiet environment, by reducing noise, dimming the lights, and limiting distractions. Next, build trust with your client by being non-judgmental and supportive in your interactions, and being an engaged listener.
Key Takeaways
Posttraumatic stress disorder (PTSD) is a mental disorder that can develop after a person is exposed to one or more traumatic events, such as sexual assault, warfare, traffic collisions, terrorism, or other threats to a person's life. It can cause a range of psychological and physical symptoms including flashbacks, nightmares, difficulty sleeping, avoidance of trauma-related cues, and alterations in how a person thinks and feels about themselves and the world. Treatment typically involves psychotherapy, medication, and support groups.