Preterm infant: Nursing
Preterm infant: Nursing
Nur 211-171 Midterm
Nur 211-171 Midterm
Notes
| PRETERM INFANT | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
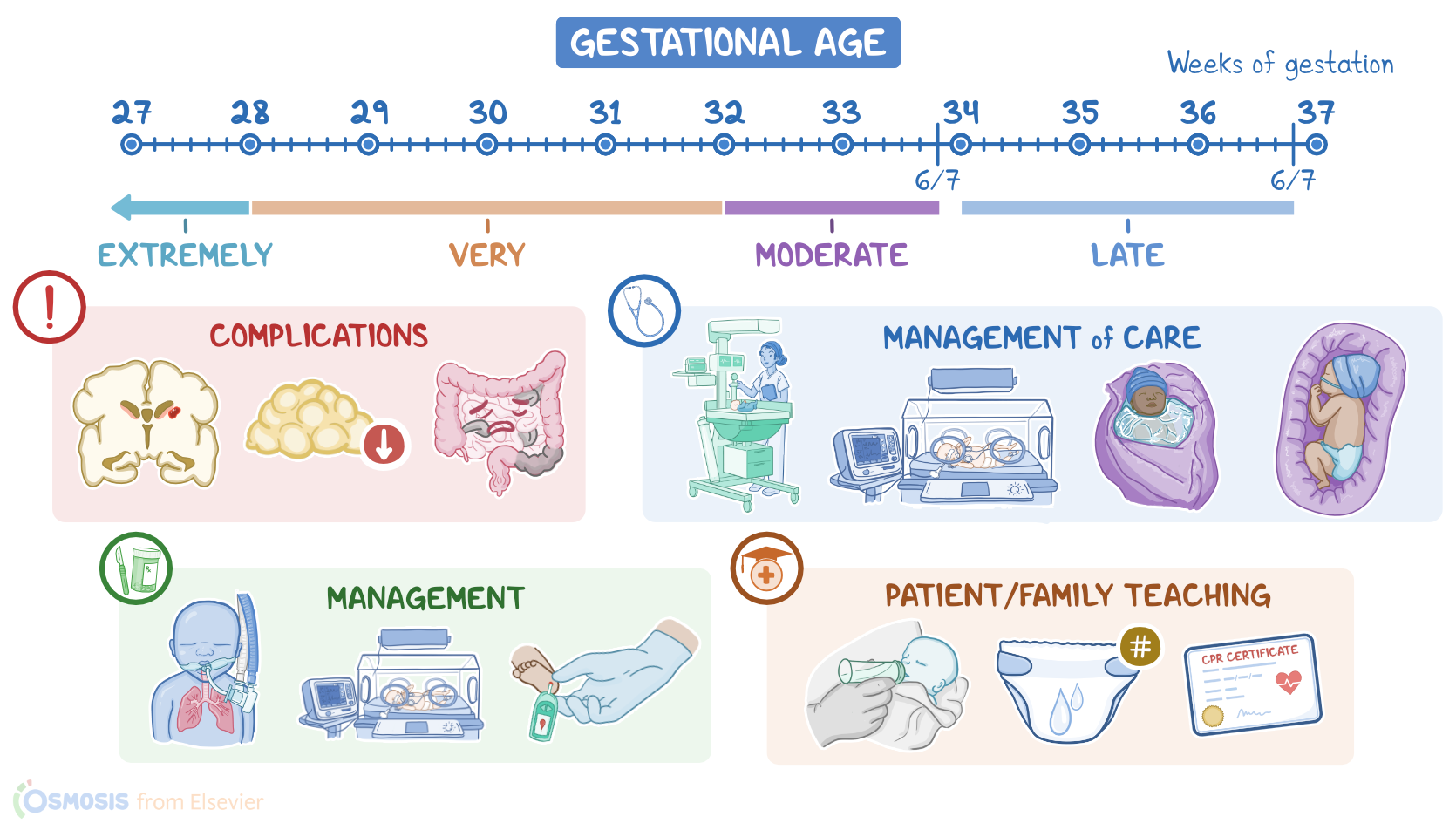
A preterm infant is born before 37 completed weeks of gestation. Classification of prematurity can be based on gestational age, so a late preterm infant is born between 34 weeks and 36 weeks and 6 days of gestation; a moderate preterm infant is born between 32 weeks and 33 weeks and 6 days of gestation;a very preterm infant is born less than 32 weeks of gestation; and an extremely preterm infant is born before 28 weeks of gestation.
Preterm infants can also be classified by birth weight. A low birth weight infant weighs less than 2500 grams; a very low birth weight infant weighs less than 1500 grams; and an extremely low birth weight infant weighs less than 1000 grams.
Let’s start with some basic physiology. Gestation refers to the period between conception and birth, which typically lasts for 40 weeks. During these 40 weeks, the embryo, and later fetus, grows and develops within the uterus.
Normally, every infant born between the 37th and 42nd week of gestation is considered a term infant, so an infant born before the 37th week is considered preterm.
Now, based on the gestational age and the infant’s birth weight, we can determine birth weight percentiles. Furthermore, birth weight percentiles help us evaluate the infant’s intrauterine growth and development, which is considered normal when the value is between the 10th and 90th percentile.
For example, an infant born at 40 weeks of gestation that weighs around 3350 grams is within the 40th percentile. In other words, this baby is appropriate for gestational age. On the other hand, an infant born at 40 weeks of gestation that weighs around 2700 grams is within the 3rd percentile, and therefore small for gestational age. Finally, an infant born at 40 weeks of gestation that weighs around 4200 grams is within the 95th percentile and is considered large for gestational age.
Now, the cause of preterm birth can be medically indicated, when there are maternal, fetal, and placental complications such as preeclampsia, fetal anomalies, or placenta previa, and is accomplished by cesarean birth or labor induction.
Preterm birth can also be spontaneous, in which case the cause is often unknown, but there are certain risk factors that can lead to premature labor and birth. These include extremes of age, like teenage pregnancy or maternal age more than 40 years of age; a history of prior preterm birth; obesity; being underweight or having a poor nutritional status; use of assisted reproductive technology like in vitro fertilization or IVF for short; cervical insufficiency; maternal substance use, including tobacco, alcohol, or illicit drugs; infections like bacterial vaginosis or an intrauterine infection; as well as factors like late or no prenatal care; high levels of stress; long working hours, especially when there’s long periods of standing; lack of social support; and intimate partner violence.
Regardless of cause, preterm infants are more likely to develop severe or life threatening complications, and the complications are more severe as gestational age and birthweight decreases.
Respiratory complications are common, and are mostly related to insufficient surfactant production. This prevents the alveoli from expanding completely, resulting in hypoxia and respiratory distress syndrome or RDS for short.
Other respiratory complications include transient tachypnea of the newborn or TTN for short, because of decreased absorption of fetal lung fluid and subsequent decreased gas exchange; pulmonary hemorrhage; apnea with accompanying bradycardia; as well as persistent pulmonary hypertension of the newborn or PPHN for short, where pulmonary pressure remains high, resulting in continued shunting of blood away from the lungs through a patent ductus arteriosus, or PDA for short.
Given these complications, preterm infants may remain on prolonged mechanical ventilation. Unfortunately, mechanical ventilation can damage the lungs over time, leading to problems like bronchopulmonary dysplasia, a lung condition that can cause chronic respiratory and developmental problems, even after the baby is discharged home.
Moreover, premature infants usually require prolonged oxygen therapy, increasing the risk of retinopathy of prematurity, which can result in vision loss.
Now, neurological complications can occur due to the presence of fragile blood vessels, called the germinal matrix, that surround the ventricles in the brain and can easily bleed, causing an intraventricular hemorrhage or IVH for short. Fluctuations in cerebral blood flow from hemodynamic instability that often occurs in preterm infants increases the risk of IVH, and can result in long-term complications such as cerebral palsy, as well as sensory or cognitive deficits.
Other problems experienced by preterm infants include hypothermia, due to their lack of subcutaneous fat, their relatively large body surface-to-weight ratio, and a decreased ability to generate heat due to absent or low levels of brown fat; hypoglycemia due to insufficient glycogen stores and increased glucose needs; an increased risk of infection due to an immature immune system and lack of IgG antibodies, which are normally transferred transplacentally around 34 weeks of gestation; as well as fluid and electrolyte imbalance, anemia, and hyperbilirubinemia.
Finally, because premature infants have an underdeveloped gastrointestinal system, they are more at risk for necrotizing enterocolitis or NEC for short, which includes inflammation, ischemia, and necrosis of the bowel.
Clinical manifestations of a preterm infant vary depending on their gestational age and birth weight, however some common ones include a disproportionately large head compared to the rest of the body, and thin extremities and lack of subcutaneous fat. Skin can be gelatinous or transparent, with opacity increasing with gestational age.
As far as behavior, preterm infants are often lethargic, but can also be jittery, easily stressed by external stimuli, and difficult to soothe. They typically have an increased respiratory effort, and a murmur is often heard at the upper left sternal border if a PDA is present. Other findings include temperature instability, a weak suck, and poor feeding.
The management of preterm infants typically includes supportive care in the neonatal intensive care unit, and includes providing respiratory support, promoting a stable temperature, and maintaining glucose levels in the normal range. Additionally, it’s important to prevent complications and treat them, if they do occur.
In general, the preterm infant is ready for discharge when they are physiologically stable; when they can coordinate their suck, swallowing, and breathing and are feeding without difficulty; when their weight stabilizes; and there are no medical conditions that require treatment in the hospital.
Now let’s talk about the nursing care you’ll be giving to a preterm infant. Your priority nursing goals are to provide supportive care, monitor for complications, and provide psychosocial support.
Begin your supportive care by ensuring your client is in a neutral thermal environment. Immediately after delivery, place the infant under a radiant warmer or in an isolette, and closely monitor their temperature.
If the infant is very premature, place them in a polyethylene bag to retain heat and moisture. Also, keep their head covered with a cap, and prewarm linens and any equipment that will be used to care for the infant.
Next, be sure to provide a therapeutic environment by positioning the infant in a flexed, tucked position, and using boundaries to provide containment.
Ensure there is minimal stimulation from light and noise, and cluster your care activities to provide adequate periods of rest.
Monitor for signs of stress, including hiccupping, splaying fingers, yawning, or grimacing, and pause your activities when possible, if you notice these signs.
Also promote comfort by offering opportunities for non-nutritive sucking, as tolerated.