Prostate cancer: Nursing
Prostate cancer: Nursing
Watch later
Watch later
Notes
| PROSTATE CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Prostate cancer is a malignant tumor that originates in the prostate gland and is the most common cancer and the second most common cause of cancer death among clients assigned male at birth.
Now, let’s quickly review the anatomy and physiology of the prostate gland. The prostate is a small gland that sits under the bladder and in front of the rectum. It can be divided into four zones. The peripheral zone, which is the outermost posterior section and is the largest of the zones, containing about 70% of the prostate’s glandular tissue. Moving inward, the central zone contains about 25% of the glandular tissue. Then there is the transitional zone, which contains around 5% of the glandular tissue, and lastly is the periurethral zone, surrounding the prostatic urethra.
Now, the prostate gland secretes the prostatic fluid, which is a slightly alkaline, milky fluid that has nutrients that nourish the sperm, enhance its movement, and help it survive in the acidic environment of the vagina. To do that, the prostate cells rely on stimulation from androgens for survival, such as testosterone produced by the testes.
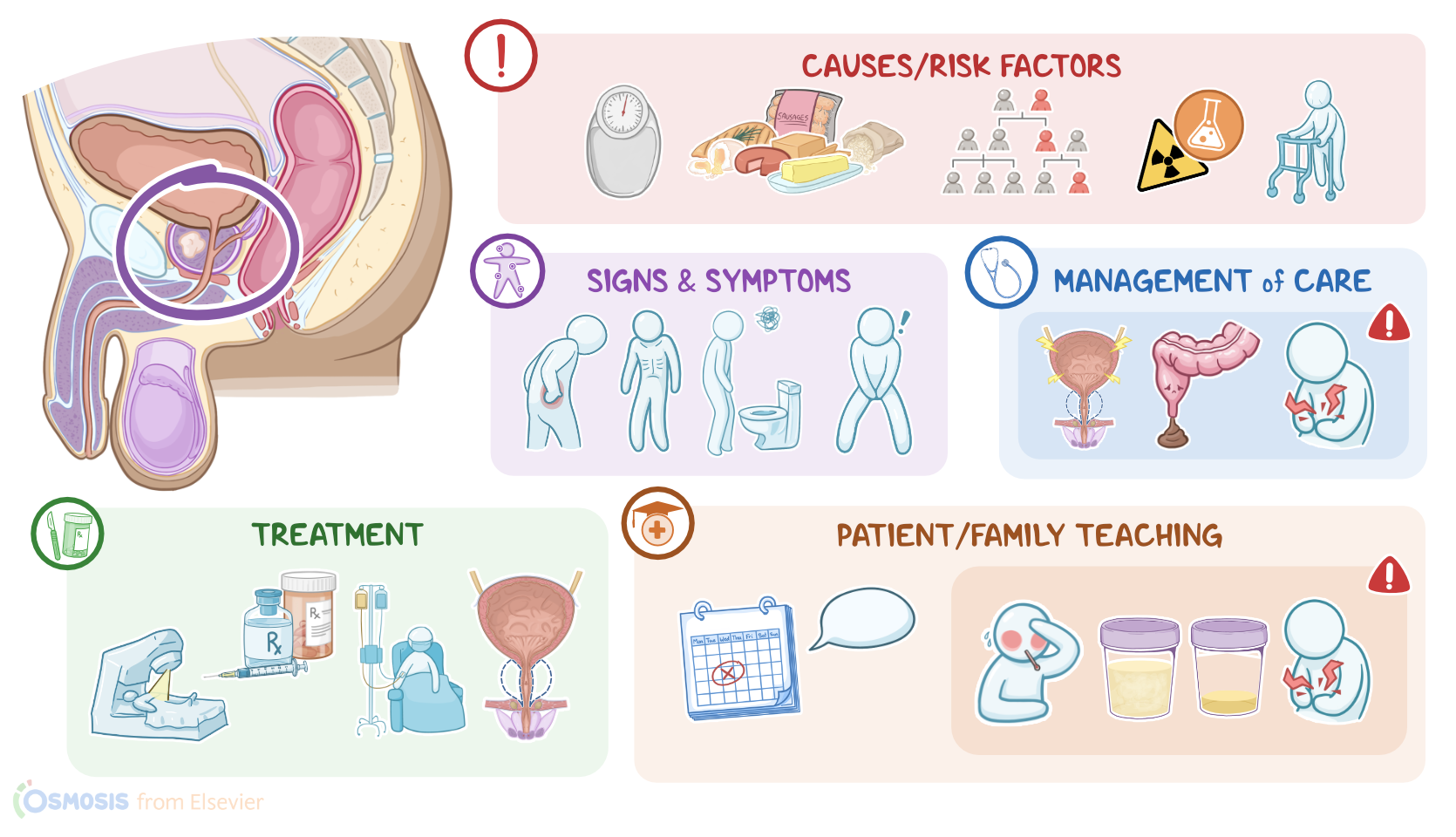
All right, now prostate cancer is typically caused by a genetic mutation in a prostate cell, such as a mutation in breast cancer genes 1 and 2, also known as BRCA1 and BRCA2 genes. These mutations may arise from a variety of risk factors. Non-modifiable risk factors include advanced age, having a family history of prostate cancer, as well as being Black. On the other hand, modifiable risk factors include obesity, a diet high in animal fat and low in fiber and vegetables, and long-term exposure to ionizing radiation or certain chemicals, such as benzene and toluene.
So, once a prostate cell becomes mutated and cancerous, it starts dividing uncontrollably, forming a tumor mass. Early on, prostate cancer cells depend heavily on androgens for survival, but eventually, the cancer cells mutate and find a way to keep multiplying without relying on androgens. Overall, prostate cancer cells have a relatively slow rate of growth compared to other types of cancers. However, as they grow they can lead to enlargement of the prostate gland and constriction of the prostatic urethra. Eventually, cancerous cells start invading neighboring tissues, and may even spread to nearby lymph nodes or metastasize to distant organs, such as the bones of the axial skeleton.
In the early stages, prostate cancer typically causes no symptoms. That’s because the majority of prostate cancers arise in the posterior peripheral zone, which is far away from the urethra. As a result, these tumors can grow quite large before they cause problems with urination. Over time, if the tumor does compress or invade the urethra or bladder, it can cause difficulty urinating, bleeding, and pain with urination and ejaculation. If the cancer metastasizes to bones, like the vertebrae or pelvis, clients can experience hip or lower back pain, and it can also lead to weight loss.
Diagnosis of prostate cancer starts with history and physical assessment, which includes digital rectal examination, or DRE for short. This is where a finger is inserted into the rectum to feel against the anterior wall of the rectum which lies along the posterior part of the prostate. Normally, the prostate feels soft and rubbery; while with prostate cancer, the prostate could feel firm, and nodules are often palpated. But if the tumor arises elsewhere, like in the anterior peripheral zone, then the tumor would be out of reach during the digital rectal exam.
Another approach is to use either a transrectal ultrasound or an MRI to image the prostate. Prostate cancer can also cause an elevation in tumor markers like prostate specific antigen or PSA for short. But ultimately, confirmation of the diagnosis of prostate cancer requires a prostate biopsy; and based on how abnormal the cancer cells appear under the microscope, the Gleason Score is used to assess the cancer’s malignancy grade into low, medium, or high. Pelvic MRI and bone scans are also done to look for metastases. Lastly, the cancer is staged by combining the TNM system that looks at the extent of the primary tumor, and whether it has spread to lymph nodes or metastasized; as well as the PSA level at the time of diagnosis; and the Gleason score.
In terms of treatment, when the tumor is confined to the prostate and hasn’t metastasized, surgical excision of the prostate, also known as prostatectomy, is frequently done. This is often accompanied by radiation therapy and hormonal therapy, which includes the use of androgen receptor blockers or inhibitors of androgen synthesis. Less commonly, an orchiectomy can be performed, where the testes are removed in order to reduce prostate stimulation from androgens.
Sometimes clients with low-stage non-metastatic prostate cancer might decide to undergo active surveillance instead since prostatectomy can cause certain complications, like damaging the prostatic plexus, resulting in erectile dysfunction, as well as urinary incontinence. Active surveillance includes routine tumor marker measurement as well as digital rectal examination and imaging, to ensure that the prostate cancer remains confined to the prostate. If the tumor has metastasized, however, treatment options include chemotherapy, and hormonal therapy; as well as radiation therapy, which can however, cause complications like radiation proctitis, characterized by damage and inflammation of the rectum.
All right, let’s talk about nursing care for a client with prostate cancer. The priority goals are to manage your client’s symptoms, monitor for complications related to treatments, and promote quality of life.
When caring for a client who has undergone a prostatectomy, be sure to implement routine postoperative interventions, and monitor them closely for complications related to the procedure. Administer the ordered IV fluids, and perform bladder irrigation to remove blood clots from the bladder and promote drainage. Keep a close eye on your client’s urinary output and amount of bleeding present. Report to the healthcare provider if you notice signs of urinary retention, such as urine output of less than 30 mL per hour; or an increase in bright red blood and clots.