Scoliosis: Nursing
Scoliosis: Nursing
Watch later
Watch later
Notes
| SCOLIOSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
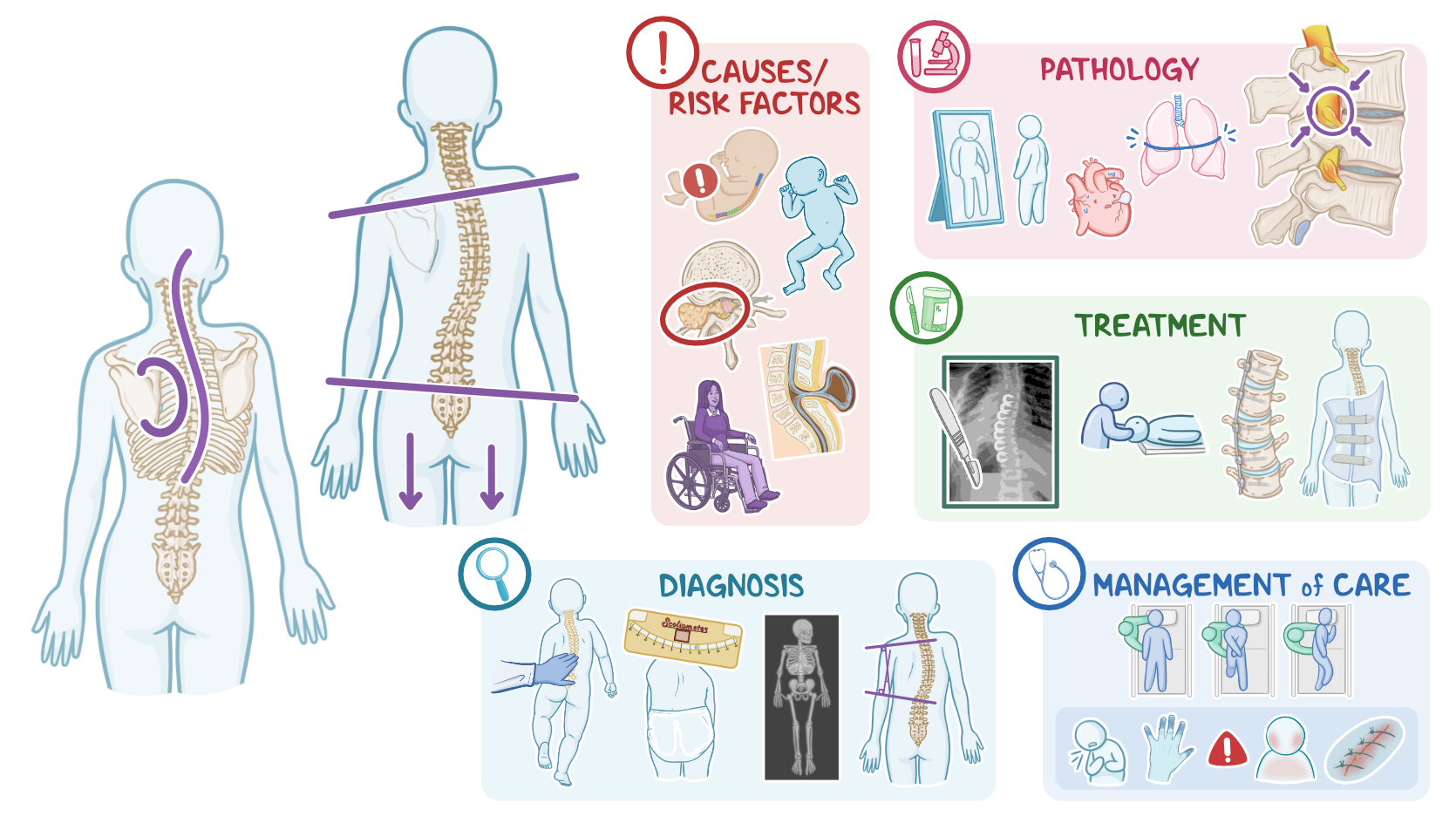
Scoliosis refers to 3-dimensional deformity of the spine, that includes a rotational and lateral, or sideways curvature of the spine that resembles an “S” or a “C” shape. Scoliosis can be idiopathic, or without known causes; congenital, or present from birth; and neuromuscular, which occurs because of some other neuromuscular condition.
First, let’s quickly review some anatomy and physiology of the spine. The bony spine, also known as the vertebral column, is made of vertebrae, and there are intervertebral discs that sit between adjacent vertebrae. These fibrocartilaginous structures act as a shock-absorbing apparatus of the spinal cord.
Now, there are 33 vertebrae, which are organized in 5 main regions: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal. Now, the cervical and the lumbar regions slightly curve inward, creating the physiologic lordosis of the spine. On the other hand, the thoracic and the sacral regions normally curve backward, which is often referred to as physiologic kyphosis. Together, the vertebrae create a bony canal that houses the spinal cord and surrounding meninges.
So, the most important functions of the spine include protection of the spinal cord and support of the head and body weight. The spine also provides the attachment of the rib cage and neighboring muscles; and allows great flexibility and motion of the trunk.
Now, based on the cause, scoliosis can be divided into three main types: idiopathic, congenital, and neuromuscular. Idiopathic scoliosis is the most common type, meaning there’s no identifiable cause. On the other hand, congenital scoliosis develops due to abnormal intrauterine development of the spine, and is present at birth. The last one is neuromuscular scoliosis, which is associated with conditions that affect the neuromuscular system. These include cerebral palsy, muscular dystrophy or atrophy, as well as spinal cord tumors and myelomeningocele, which is when the spinal cord and the surrounding meninges protrude out of an opening in the bony vertebrae into a cyst like pouch.
Now, pathology-wise, scoliosis typically becomes apparent during adolescence, because of the physiological growth spurt. So when the body grows at a faster rate, sometimes the skeletal system doesn’t keep up, resulting in skeletal deformities, such as scoliosis. In scoliosis, there is an abnormal rotation of the vertebral bodies around their vertical axis. As a result, the affected vertebral bodies rotate to the side of the spine that is curved outward, eventually causing the spine to take the shape of a letter S or C. Abnormal anatomy of the spine further causes chest deformation, rib displacement, and asymmetry of distant parts of the body.
Important complications of scoliosis include spinal stenosis, which is the narrowing of the spinal canal; radiculopathies, or pinched nerves; and altered body image that can impact the client's mental health. Additionally, abnormal anatomy of the chest can decrease pulmonary capacity and compromise respiratory as well as cardiac function. Clinical manifestations of scoliosis primarily include asymmetry of the shoulder and hip height, as well as differences in leg length. Some clients might also have one prominent shoulder blade.
Diagnosis of scoliosis includes the client’s history, and physical assessment. A scoliometer is often used, which is a small instrument that is placed over the spine while the client is bending forward at the waist, in order to measure the extent of the spinal rotation. This will then help determine whether or not a client requires further evaluation with an X-ray. The amount of spinal curvature is measured by the Cobb angle, which is determined by measuring between two lines drawn perpendicular to the upper border of the uppermost vertebrae, and the lower border of the lowest vertebrae involved in the curvature. Finally, a CT and MRI might be needed for preoperative assessment of clients who require surgical intervention.
On a side note, screening for scoliosis is commonly performed during adolescence. Screening tests include visual inspection of the spine and back, as well as palpation of the spine to check for abnormal curvatures, as well as the forward bend test, which can be done with or without a scoliometer.
Treatment is based on several important factors, including the client’s age, their predictive growth, presence of other conditions, and finally, the degree and location of the curvature. Minor curvatures, meaning less than 25 degrees, can benefit from physical therapy, which helps prevent their progression. Curvatures that range from 25 to 40 degrees also don’t require surgical intervention, but they’re instead treated with thoracic lumbar sacral orthosis, which is a type of bracing, meaning a stiff torso armor that helps slow the progression of the abnormal curvature.
On the other hand, a curvature beyond 45 degrees typically requires a surgical intervention, such as stapling. Stapling is something like having braces for the teeth but on the spine. If scoliosis continues to progress, alternative surgical interventions, such as body tethering and spinal fusion, can be considered. In body tethering, a small flexible cord is inserted next to the spine to connect adjacent vertebrae and preserve their mobility. Similarly, in spinal fusion, there’s a surgical fusion of two or more adjacent vertebrae, but with steel rods, therefore the spine’s flexibility is less preserved when compared to body tethering.
Alright, now let’s look at the nursing care you’ll provide for a client with scoliosis. Your priority nursing goals are to monitor for cardiopulmonary complications, provide supportive care during treatment, and provide psychosocial support.
Okay, begin by assessing your client’s vital signs, and auscultating their lung and heart sounds. Take note of any signs or symptoms of cardiopulmonary compromise, and immediately report if your client is experiencing dyspnea or chest pain; or if you note blue-tinged extremities, increased blood pressure, or increased pulse.
Now, if your client is prescribed a brace, measure and record your client’s shoulder levels, and the heights of their anterior and posterior superior iliac spines, to help monitor the progression of their spinal curvature. Also, collaborate with the physical therapist to provide exercises to promote strength, posture alignment, and balance, as prescribed.
Key Takeaways
Scoliosis is an abnormal lateral curvature of the spine that resembles an S � or C � shape. The cause of scoliosis is usually unknown, but it may result from abnormal intrauterine spine development, as well as from certain diseases like cerebral palsy, muscular dystrophy, spinal cord tumors, and myelomeningocele.
Complications of scoliosis include spinal stenosis, radiculopathies, pinched nerves, cardiac and respiratory compromise, and altered body image that can impact the client's mental health. People with scoliosis can present with asymmetry of the shoulder and hip height and leg discrepancy.
The diagnosis involves the use of a scoliometer to measure spinal rotation, and an x-ray to measure the Cobb's angle. Treatment may include physiotherapy, or surgery such as stapling, body tethering, or spinal fusion. Nursing management focuses on monitoring cardiopulmonary complications, providing supportive care during treatment, and providing psychosocial support.