Strabismus: Nursing
Notes
| STRABISMUS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Contributors
Strabismus is a common condition characterized by misalignment of the eyes due to a lack of eye muscle coordination. Strabismus can present occasionally or constantly, and is commonly referred to as crossed eyes or squint.
Let’s start with some basic anatomy and physiology. Eye movement is controlled by the six extraocular muscles, which include four rectus muscles and two oblique muscles. The rectus muscles are the superior rectus, which moves the eye upwards; the inferior rectus, which moves the eye downwards; the medial rectus, which moves the eye medially; and the lateral rectus, which moves the eye laterally. The last two are the superior and inferior oblique muscles, which control the rotation of the eyeball.
These extraocular muscles are innervated by cranial nerves that arise directly from the brain. More specifically, the abducens nerve, or cranial nerve VI, innervates the lateral rectus muscle; the trochlear nerve, or cranial nerve IV, innervates the superior oblique; and lastly, the oculomotor nerve, or cranial nerve III, innervates the rest of the extraocular muscles. Typically, control of eye movement should have developed completely by 4 months of age.
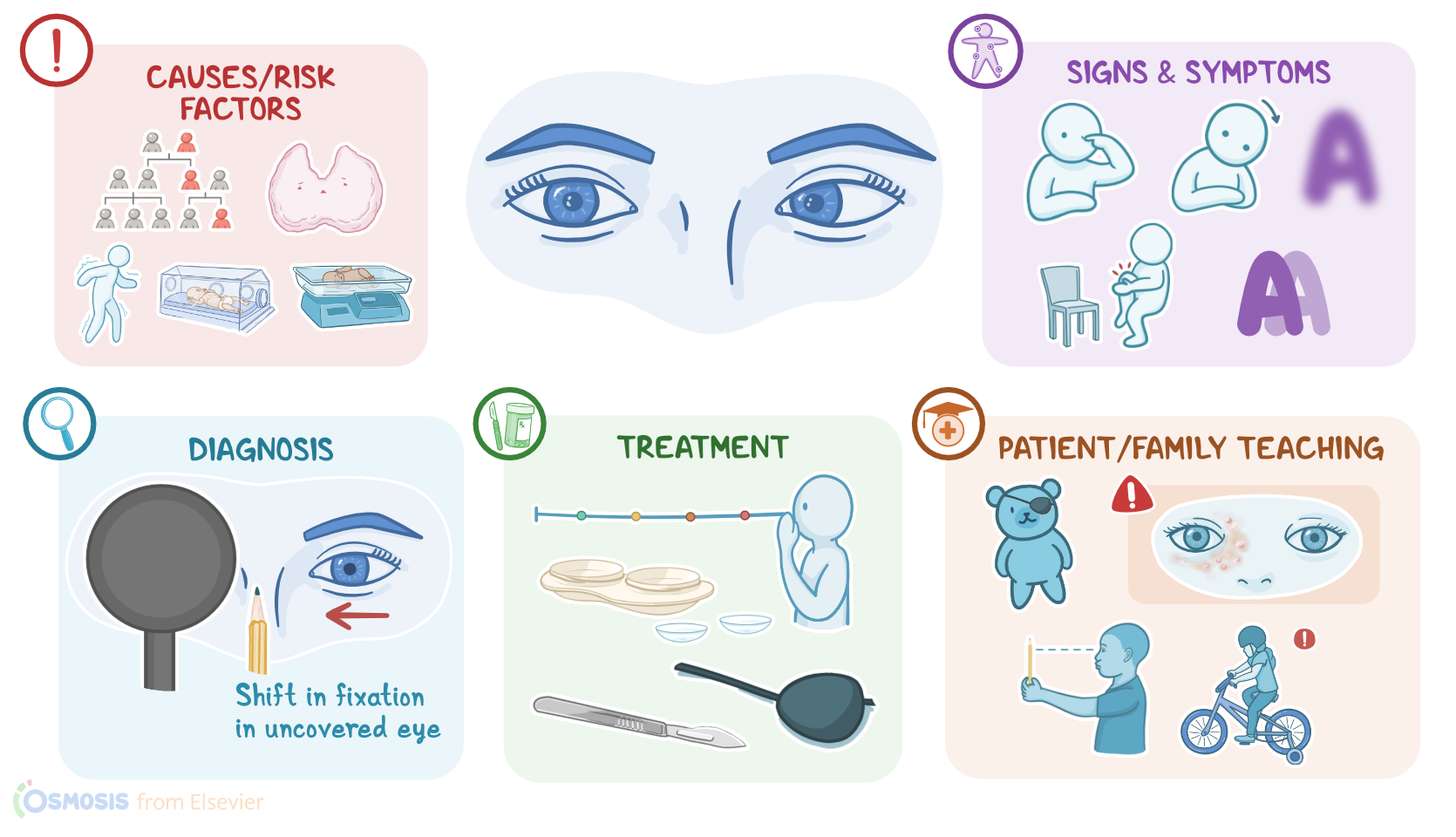
Now, strabismus can be caused by problems involving the brain centers controlling eye movements, the cranial nerves that supply the muscles, or less commonly, the muscles themselves. This includes cranial nerve palsy, which is characterized by impaired function leading to weakness or even paralysis of the innervated muscle; as well as cerebral palsy, head trauma, or strokes. Strabismus can also be caused by sensory deviation due to eye conditions like refractive errors, cataract, retinal detachment, or retinoblastoma. Less frequently, strabismus has congenital causes, such as Down syndrome. Finally, when the cause is unknown, strabismus can also be idiopathic.
These conditions can also be considered risk factors for strabismus, along with family history, thyroid disease, neuromuscular disorders, prematurity, and low birth weight.
Alright, now regardless of the underlying cause, the pathology of strabismus is characterized by misalignment of one eye, as well as a lack of eye coordination, which means that both eyes are unable to focus on one object at the same time. Now, to avoid double vision, also called diplopia, the brain ignores the images received from the misaligned eye, and may only focus on the stronger eye. Over time, this may cause the misaligned eye to get progressively weaker, which causes visual deficits and amblyopia.
The typical clinical manifestations of strabismus include uncoordinated eye movements, as well as eyes that don’t aim in the same direction.
Strabismus can be classified according to the direction of the misaligned eye into four categories: exotropia, in which the misaligned eye turns outward; esotropia, in which the misaligned eye turns inwards; hypertropia, in which the misaligned eye turns upwards; and hypotropia in which the misaligned eye turns downwards. Additionally, clients often have diplopia, blurred vision, tired eyes, and headaches; in addition to squinting or closing one eye, or tilting the head to focus on a single object. Some clients can also report bumping into objects due to reduced sense of depth.
Also, clients can have intermittent strabismus, where the eyes are misaligned only part of the time. When the eye muscles are tired, like at the end of the day or during an illness, it may become more pronounced.
The diagnosis of strabismus starts with the client's history and physical assessment. Ideally, a child’s ocular alignment should be assessed between 4 to 6 months of age to identify strabismus and other ophthalmic problems so they can be treated early.
Diagnostic tests include a corneal light reflex test is done by holding a penlight 1 to 2 feet from the child’s face while they are looking at a small toy or picture. If the reflection of the light is symmetrically centered on the cornea in each eye, no strabismus is present. If the light reflex is misaligned in 1 eye, then strabismus is likely.
The cover test can also be done, by asking the client to fix their eyes on a single object, then covering one eye while observing the other eye’s movement; the test is repeated on the opposite eye. Ocular alignment is normal if no movement is detected in the uncovered eye; and strabismus is confirmed if there’s a shift in fixation of the uncovered eye.
The treatment of strabismus includes non-surgical and surgical options. Non-surgical options involve corrective lenses and occlusion therapy, which is when the stronger eye is covered to force the brain to receive images from the misaligned eye, making it stronger. Visual training exercises that help the brain and eyes work effectively together can also be tried.
Key Takeaways
Strabismus is a common condition characterized by misalignment of the eyes due to a lack of eye-muscle coordination. Strabismus can present occasionally or constantly and is commonly referred to as crossed eyes or squint.
Strabismus is caused by a variety of factors, such as conditions affecting cranial nerves III, IV, and VI, or the muscles controlling the eye, or other problems in the brain. Risk factors include family history, neuromuscular disorders, prematurity, and low birth weight. Symptoms of strabismus include uncoordinated eye movements and eyes that don't aim in the same direction, and there may also be blurred vision, tired eyes, headaches, squinting, head tilting, or a tendency to bump into objects.
Treatment for strabismus usually involves glasses, visual training exercises, and surgery. Nursing management includes providing supportive care during treatment and monitoring for adherence to the treatment plan. Client and family education emphasizes treatment adherence and when to contact the healthcare provider.