Case study - Pressure injury prevention: Nursing
Notas
| CASE STUDY - PRESSURE INJURY PREVENTION | ||
| KEY POINTS | MY NOTES | |
| INTRODUCTION |
| |
| RECOGNIZING AND ANALYZING CUES |
| |
| PRIORITIZING HYPOTHESE, GENERATING SOLUTIONS, AND TAKING ACTION |
| |
| EVALUATING OUTCOMES |
| |
Transcripción
Revisores de contenido
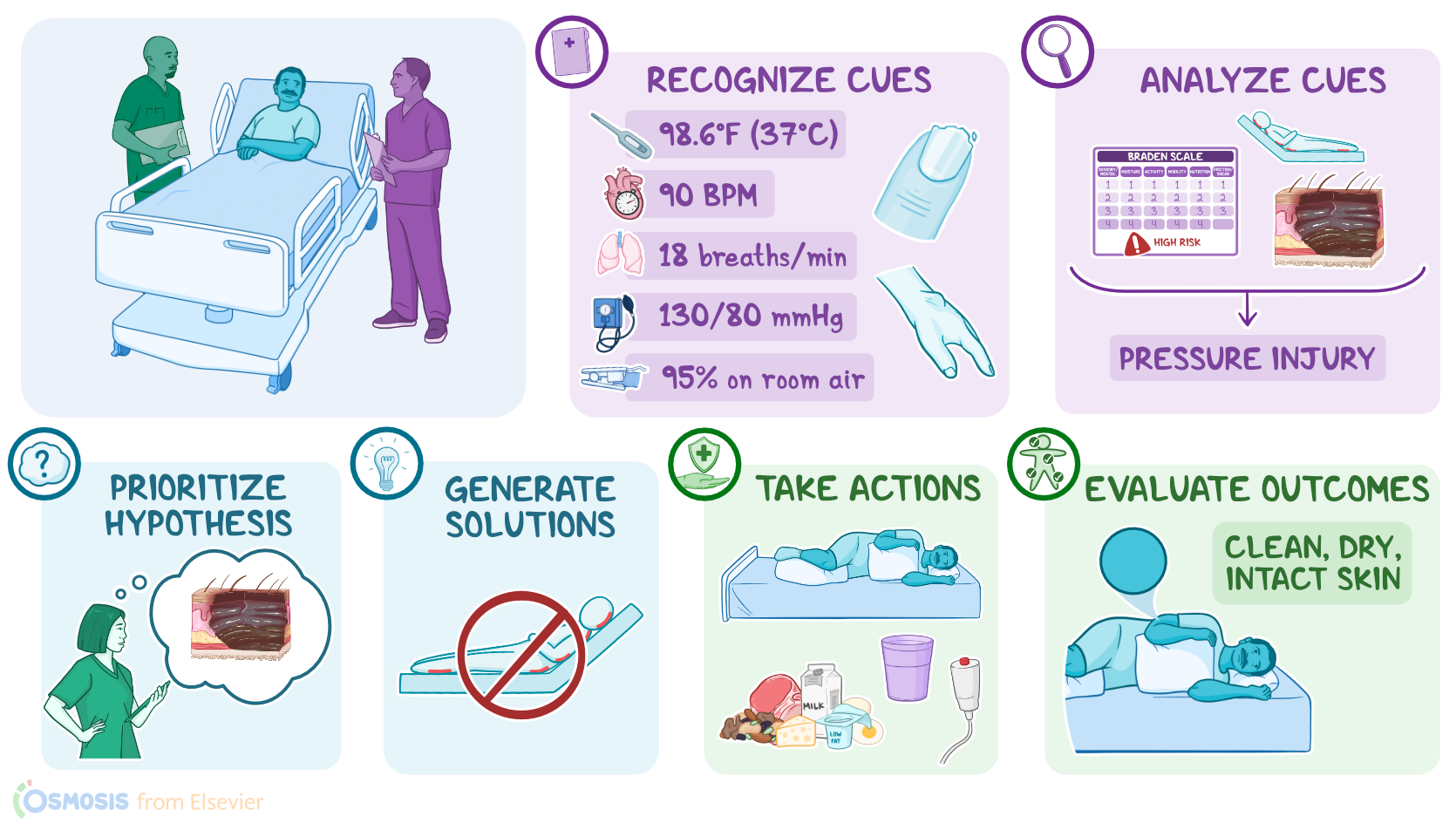
Nurse Nathan works at a rehabilitation hospital and is caring for Larry, a 72-year-old with a left below-the-knee amputation related to complications from diabetes mellitus. In collaboration with the registered nurse, RN Ashmeet, Nurse Nathan goes through the steps of the Clinical Judgment Measurement Model to make clinical decisions about Larry’s care by recognizing and analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes.
First, Nurse Nathan recognizes important cues, including Larry’s vital signs, which are
temperature of 98.6 F or 37 C, heart rate 90 beats per minute, respirations 18 breaths per minute, blood pressure 130/80 mmHg, and oxygen saturation 95 percent on room air. Nurse Nathan notes that Larry has been incontinent of urine and is struggling to effectively reposition himself in bed. Nurse Nathan also notices that Larry has clinical signs of malnourishment such as dry, thin skin and brittle nails and hair.
Next, Nurse Nathan analyzes these cues. He reviews the electronic health record, or EHR, and notes that Larry developed a pressure injury on his sacrum during a past hospitalization that has since healed. He also sees that RN Ashmeet calculated Larry’s pressure injury risk using the Braden Scale which indicated that Larry is at high risk for developing another pressure injury.
Nurse Nathan understands that pressure injuries involve damage to the skin or underlying tissue because of prolonged pressure, which causes reduced blood flow. This results in tissue hypoxia and ischemia, which ultimately leads to necrosis and ulceration. Nurse Nathan knows that most often, pressure injuries develop in patients who have difficulty moving around or are totally immobile. He also knows other factors increase the risk for pressure injury, like thinning of skin and subcutaneous tissue due to age and impaired nutrition and hydration; exposure to skin irritants, like urine; as well as diabetes mellitus which can impair blood flow. Nurse Nathan realizes Larry needs effective pressure injury prevention.
Now, using the information he has gathered, along with Larry’s medical history, Nurse Nathan discusses his findings with RN Ashmeet, and they choose a priority hypothesis of risk for impaired skin integrity.
Then, they generate solutions to address Larry’s risk for impaired skin integrity, and they establish the expected outcome that after intervening, Larry will not develop a pressure injury during the shift.
Nurse Nathan then takes action to implement these solutions. He starts by working with the unlicensed assistive personnel to keep Larry clean and dry and apply barrier cream to his groin and buttocks. They also change the sheets and ensure there are no wrinkles in the bedding that could cause friction and irritate Larry’s skin. They use pillows to reposition Larry on his left side and elevate his heel and elbows off the bed. Then, Nurse Nathan sets an alarm as a reminder to reposition Larry again in two hours.
RN Ashmeet also speaks with the health care provider who orders protein shakes to enrich Larry’s diet and a pressure relieving mattress for Larry. RN Ashmeet also teaches Larry about the importance of consuming protein-rich foods to promote skin integrity. After RN Ashmeet leaves the room, Nurse Nathan re-enters the room to give Larry the protein shake and reinforce teaching.
Fuentes
- "Foundations of nursing. (9th ed.). " Elsevier. ISBN: 9780323827119 (2023)
- "Fundamental concepts and skills for nursing. (6th ed.). " Elsevier. ISBN: 9780323694780 (2022)