The causes of fetal decelerations mainly depend on the types of decelerations.
Early decelerations in FHR are caused by compression of the fetus’s head during a uterine contraction. As the uterine muscles get tighter and shorter, the size of the uterus decreases, thereby limiting the available space for the fetus. Especially a few weeks before labor, when the baby is tightly fitted in the uterus, the pressure applied to the fetus during uterine contractions may bend the fetus’s neck, causing vagal stimulation. Stimulation to the vagus nerve can cause a decrease in the FHR seen as a deceleration that disappears immediately after the contraction. These decelerations are completely benign as they do not affect fetal oxygenation and, therefore, do not require treatment.
Late decelerations are caused by uteroplacental insufficiency, which is a decrease in the blood flow to the placenta that reduces the amount of oxygen and nutrients transferred to the fetus. Any condition that predisposes decreased uteroplacental blood flow can cause late decelerations. Some triggering circumstances include low maternal blood pressure (i.e., hypotension) from the epidural analgesia, dehydration of the mother, anemia of the mother, rapid uterine contractions, placental abruption (i.e., the early separation of the placenta from the uterus before labor), and fetal hypoxia (i.e., low oxygen levels).
Lastly,
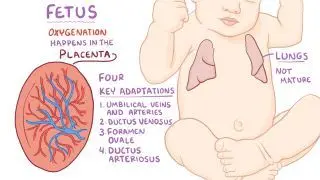
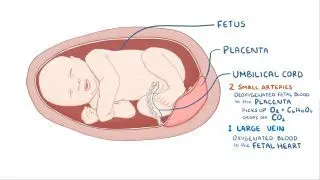
variable decelerations are caused by compression of the
umbilical cord. Pressure on the cord initially occludes the
umbilical vein, which results in an acceleration (i.e., an increase of the FHR) and indicates a healthy response. This is followed by occlusion of the umbilical artery, which results in a sharp deceleration as the fetal blood supply is suddenly restricted. Decreased
amniotic fluid during pregnancy (i.e.,
oligohydramnios) is associated with more frequent variable decelerations as the amniotic fluid has a protective role on the fetal umbilical cord.