
A woman arrives for her postpartum visit and reports a variety of mental health symptoms like anxiety and irritability. What are the next steps determining a diagnosis? Do you know? Let’s find out!
A 27-year-old G3P1112 woman presents for a 6-week postpartum visit. The patient had an uncomplicated repeat cesarean delivery following a pregnancy complicated by gestational diabetes managed with diet and exercise. There is a history of preterm delivery at 34 weeks due to preterm rupture of membranes with cord prolapse that required an emergent cesarean delivery. Since delivery, the patient reports excessive anxiety and worry, along with irritability, restlessness, fatigue, and difficulty concentrating. Similar symptoms occurred after the first delivery but resolved after six months without intervention. The patient reports no other history of anxiety or depression. Vital signs are within normal limits, and a chaperoned examination is unremarkable.
Which of the following is the most likely diagnosis?
A. Postpartum blues
B. Perinatal depression
C. Postpartum psychosis
D. Perinatal anxiety
E. Bipolar disorder
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
D. Perinatal anxiety
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Postpartum blues
Incorrect: Mild perinatal depression, or postpartum blues, typically occurs within 2 days up to 2 weeks after delivery. Symptoms include dysphoric mood, crying, mood lability, anxiety, sleeplessness, loss of appetite, and irritability. This patient’s symptoms have persisted beyond 2 weeks and are more consistent with perinatal anxiety.
B. Perinatal depression
Incorrect: Although fatigue and concentration difficulties are present, the predominant symptoms—excessive anxiety, worry, restlessness, and irritability—align more with perinatal anxiety. Continued monitoring is advised, as perinatal anxiety can be a predictor for perinatal depression.
C. Postpartum psychosis
Incorrect: Postpartum psychosis is rare but serious. Symptoms can include agitation, delusions, disorganized thoughts, bizarre behavior, auditory or visual hallucinations, and intrusive thoughts of suicide or infanticide. None of these features are evident here, and the patient’s presentation is more consistent with perinatal anxiety.
E. Bipolar disorder
Incorrect: While it’s important to rule out bipolar disorder before starting medication for perinatal depression and anxiety, this patient does not have a history of manic or hypomanic episodes consistent with this diagnosis.
Main Explanation
Perinatal anxiety is the most likely diagnosis based on the patient’s symptoms of excessive anxiety and worry, irritability, restlessness, and difficulty concentrating for more than two weeks. A standardized screening tool, such as the General Anxiety Disorder-7 (GAD-7) or Edinburgh Postnatal Depression Scale (EPDS) with positive anxiety indicators, can aid in confirming the diagnosis.
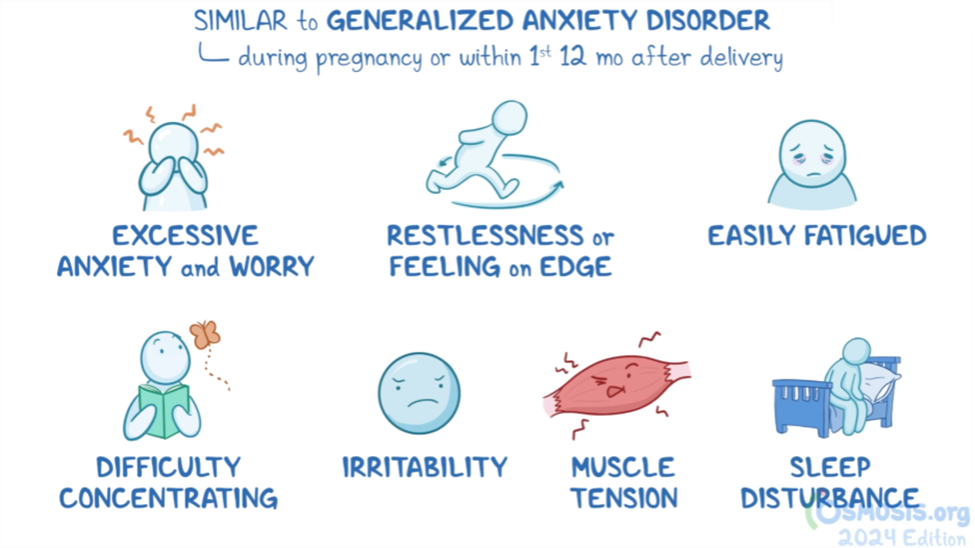
Patients with perinatal anxiety present during pregnancy or within the first 12 months after delivery with symptoms similar to generalized anxiety disorder. These symptoms include excessive anxiety and worry along with at least three of the following: restlessness or feeling on edge, fatigue, difficulty concentrating or a mind that goes blank, irritability, muscle tension, or sleep disturbances. Risk factors include personal or family history of anxiety, prior pregnancy loss, an unplanned or complicated pregnancy, intimate partner violence, or a history of childhood abuse.
Perinatal anxiety is a predictor for perinatal depression. Treatment includes self-care measures such as adequate sleep, exercise, and balanced nutrition. Both psychotherapy and pharmacotherapy are effective first-line treatments, with added benefits when used together. Psychotherapy includes cognitive behavioral therapy (CBT) and interpersonal psychotherapy (IPT). The preferred pharmacotherapy is selective serotonin reuptake inhibitors (SSRIs); sertraline is often preferred, although escitalopram is an acceptable alternative. Serotonin-norepinephrine reuptake inhibitors (SNRIs), such as venlafaxine, can also be used. While benzodiazepines are often used for anxiety outside of pregnancy, they should be used sparingly in perinatal anxiety and only as a temporary bridge until psychotherapy, SSRIs, or SNRIs take full effect. A collaborative treatment approach may involve a mental health professional and, if indicated, hospitalization.
Major Takeaway
Perinatal anxiety presents with symptoms similar to generalized anxiety disorder and is diagnosed during pregnancy or within the first 12 months after delivery. Symptoms include excessive anxiety and worry, along with at least three of the following: restlessness or feeling on edge, fatigue, difficulty concentrating or a mind that goes blank, irritability, muscle tension, or sleep disturbances.
Want to learn more about this topic?
Watch the Osmosis video: Perinatal depression and anxiety: Clinical sciences
References
- American College of Obstetricians and Gynecologists. Practice Advisory: Zuranolone for the Treatment of Postpartum Depression. January 30, 2024. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2023/08/zuranolone-for-the-treatment-of-postpartum-depression
- American College of Obstetricians and Gynecologists’ committee on clinical practice guidelines-obstetrics. ACOG clinical practice guideline no 4. Screening and diagnosis of mental health conditions during pregnancy and postpartum. Obstet Gynecol. 2023;141(6):1232-1261. doi:10.1097/AOG.0000000000005200
- American College of Obstetricians and Gynecologists’ committee on clinical practice guidelines-obstetrics. ACOG clinical practice guideline no 5. Treatment and management of mental health conditions during pregnancy and postpartum. Obstet Gynecol. 2023;141(6):1262-1288. doi:10.1097/AOG.0000000000005202

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply