
Today, we’re examining a clinical case of a 77-year-old woman arrives at the ED for an evaluation of pain and increased irritability over a period of three days. What’s the most likely diagnosis? Do you know the answer? Let’s find out!
A 77-year-old woman was brought to the emergency department from a nursing home for evaluation of pain and increased irritability for three days. Medical history is notable for type II diabetes mellitus, Alzheimer dementia, and a left middle cerebral artery stroke that occurred nine-years ago. The patient has limited mobility and is largely bedbound. Temperature is 37.0°C (98.6°F), blood pressure is 129/73 mmHg, and pulse is 83/min. Physical examination reveals the findings seen below in the sacral region.

Which of the following is the most appropriate management for this patient’s cutaneous findings?
A. Surgical debridement
B. Skin biopsy
C. Intravenous antibiotics
D. Negative pressure dressing
E. Cushioned dressings
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
E. Cushioned dressings
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Surgical debridement
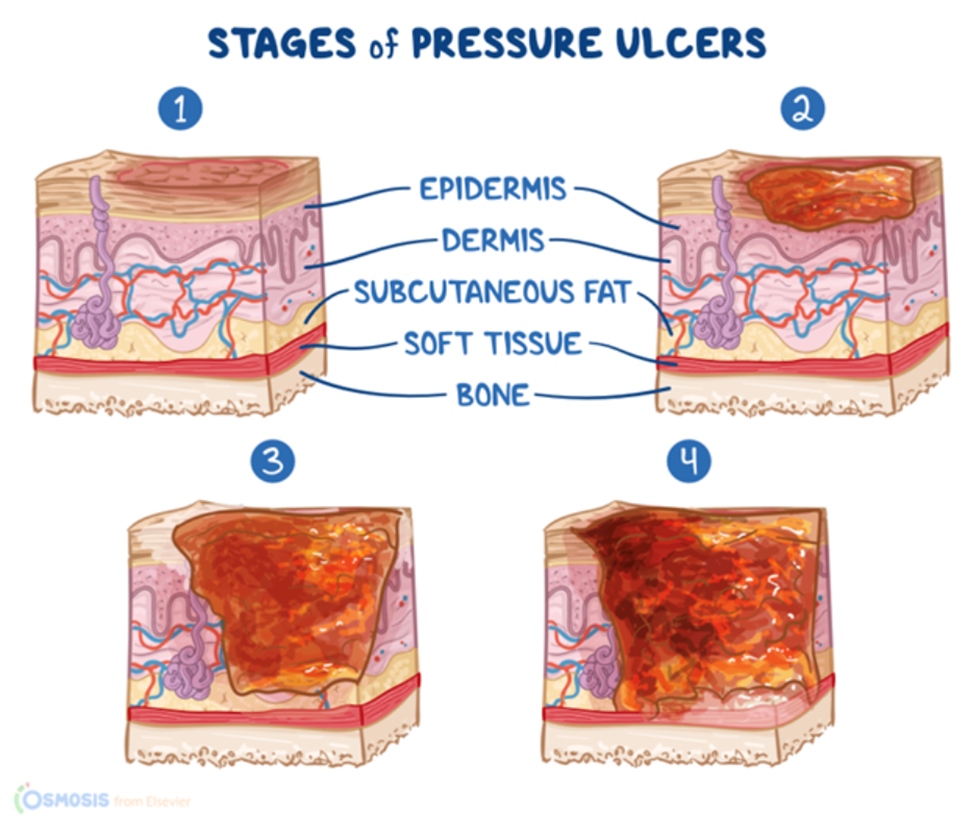
Incorrect: Surgical debridement may be indicated for the management of stage III and IV pressure ulcers or to help stage wounds that cannot be visualized due to the presence of eschar. Stage III and Stage IV pressure ulcers are characterized by full-thickness skin loss and exposure of the underlying tissue (e.g., adipose, muscle, bone). This patient’s pressure ulcer is a shallow lesion with partial thickness loss extending to the dermis. It is most consistent with a stage II pressure ulcer, which does not require surgical intervention.
B. Skin biopsy
Incorrect: Biopsy is not typically indicated in the management of pressure ulcers.
C. Intravenous antibiotics
Incorrect: Local antibiotic ointments may be indicated if there is concern for concurrent cellulitis in patients with pressure ulcers. Systemic antibiotics would not be necessary in this case given the lack of severe localized infection (e.g. osteomyelitis) or systemic infection (e.g. sepsis)
D. Negative pressure dressing
Incorrect: Negative pressure dressings help reduce bacterial growth and improve granulation tissue formation. They are used in the management of stage III and IV pressure ulcers. In contrast, this patient has a stage II pressure ulcer. Negative pressure dressings are not used in the management of stage II pressure ulcers.
Main Explanation
This patient presents with a lesion demonstrating partial loss of the dermis without exposure to subcutaneous fat, muscle, or bone. These findings are consistent with a stage II pressure ulcer, which can be managed conservatively with cushioned dressings.
Pressure ulcer management depends on its staging. Stage I (intact skin with non-blanchable erythema and no signs of necrosis) and stage II wounds (shallow, open ulcer with partial thickness loss of dermis) require local management. Treatment involves keeping the wound moist with medicated gauze and decreasing pressure and friction with cushioned dressings. If the patient is bed or wheelchair-bound, pressure on affected areas can be reduced by frequent repositioning on specialized support surfaces such as foam wedges, cushioned seating, or water beds.
Stage III (full-thickness loss of skin and exposure to subcutaneous fat) and stage IV (exposure of underlying muscle, tendon, or bone) require more invasive therapies. Deeper wounds tend to have more fibrinous exudate and necrotic tissue, which requires chemical or surgical debridement to prevent infection. Once the wound bed is clean, a negative pressure wound dressing can be applied to reduce bacterial growth and promote granulation tissue formation. Stage IV wounds heal poorly on their own and may require an autologous tissue graft.
Major Takeaway
Stage I and II pressure ulcers are managed by applying medicated dressings, cushioned dressings, and frequent repositioning. Stage III and IV pressure ulcers often require debridement, negative pressure wound dressings, and potential autologous tissue grafting.
Want to learn more about this topic?
Watch the Osmosis video: Pressure-induced skin and soft tissue injury: Clinical sciences
References
- Bluestein,D., Javaheri, A. (2008) Pressure ulcers: Prevention, evaluation, and management. American Family Physician. 78(10), 1186-1194. PMID: 19035067.

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning with us.
Leave a Reply