Acute compartment syndrome: Nursing process (ADPIE)
Notes
| ACUTE COMPARTMENT SYNDROME | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Huang Li is a 26-year-old male client who presents to the emergency department, or ED. While snowboarding this morning, Mr. Li sustained a nondisplaced transverse fracture in his right tibial shaft. A cast was applied in the ED, and he was discharged home with a prescription for the opioid analgesic acetaminophen with codeine for pain. Mr. Li came back to the ED six hours later stating his pain is unbearable with a rating of 10/10. He says the pain medication isn’t helping at all, and it feels like there are pins and needles in his leg under the cast. The ED team urgently begins evaluating Mr. Li for acute compartment syndrome.
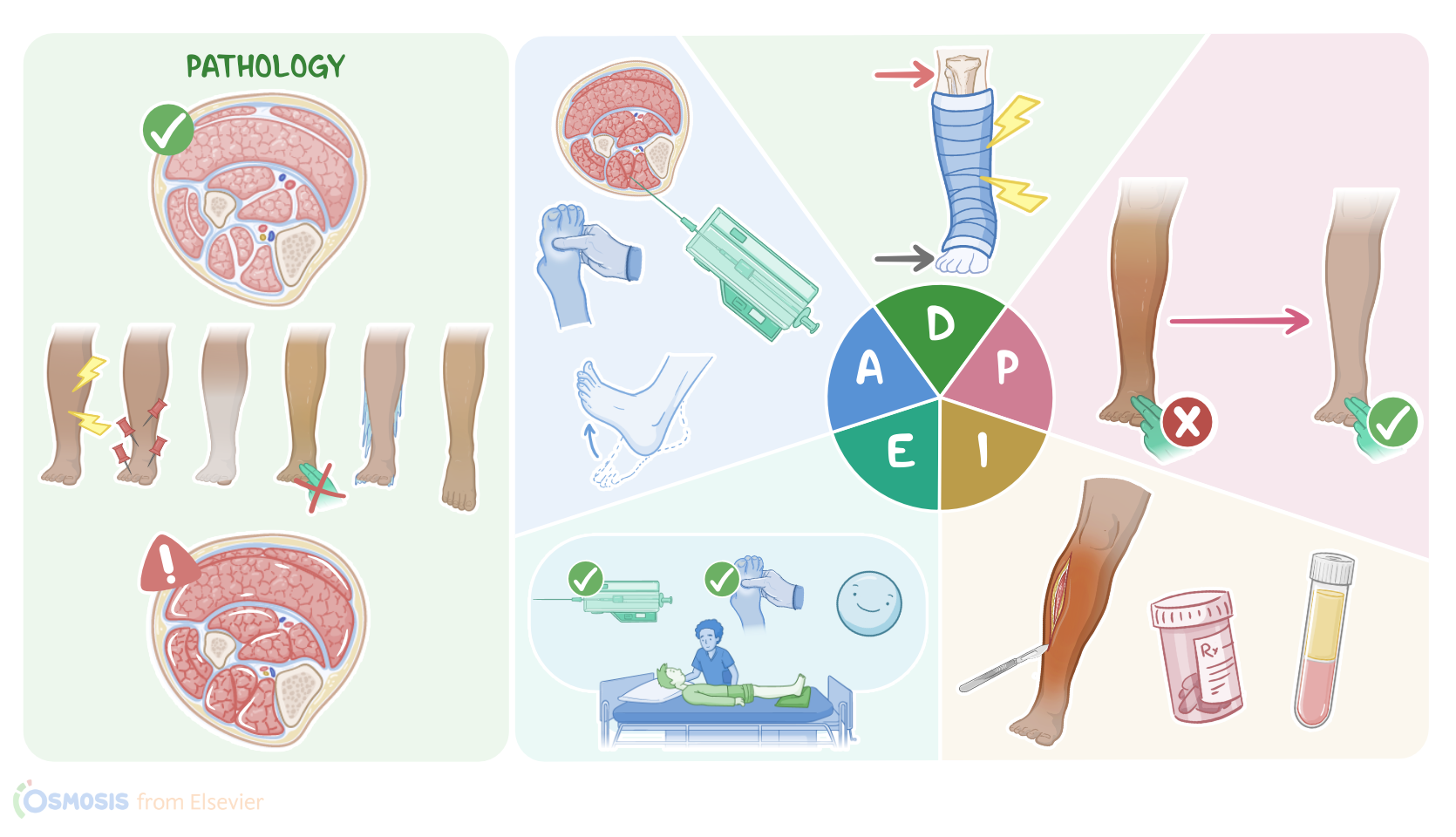
Acute compartment syndrome is a serious condition in which there’s a rapid increase in the pressure within an enclosed compartment that contains muscles, nerves, and blood vessels, surrounded by a layer of fibrous connective tissue, called fascia. Since the fascia is not elastic it can’t stretch much. So when the pressure within these compartments rises, normal blood flow can be cut off, leading to tissue damage due to hypoxia and ischemia.
The most common cause of acute compartment syndrome is bleeding within the compartment. This typically occurs with long bone fractures, like the tibia, as well as penetrating injuries. Any limb compression, like from a crush injury or severe contusion, can also lead to acute compartment syndrome. Other causes are severe circumferential burns, which can lead to tissue edema. Finally, another potential cause can be reperfusion injury in clients who experience prolonged tissue hypoxia, where a sudden restoration of blood supply can result in massive inflammation and edema.
Now, there are also some factors that may put the client at an increased risk of acute compartment syndrome, such as experiencing severe trauma, penetrating injury, motor vehicle crash, or burn injury. Acute compartment syndrome can also occur in clients who receive massive amounts of intravenous fluids, which may extravasate and infiltrate into the tissue; or those at increased risk of bleeding, such as clients with bleeding disorders, such as hemophilia, or those who take anticoagulation therapy, like warfarin. Finally, an important risk factor is compression from external factors, such as with constrictive bandages, casts, and tight dressings.
All right, acute compartment syndrome most commonly affects the legs. The typical symptoms can be remembered by the 6 Ps. The earliest two symptoms are severe Pain out of proportion to the injury; and Paresthesia, or a feeling of “pins and needles” or numbness in the affected compartment. In addition, the affected compartment will be swollen and very stiff, like a piece of wood. If not promptly treated, clients may develop the next 3 Ps, which are Pallor, Pulselessness, where the distal arterial pulses become very weak or even absent, and Poikilothermia, which refers to coolness of the affected area. The last P stands for Paralysis, which is rare and suggests extensive damage to both the muscles and nerves.
Acute compartment syndrome can lead to serious long-term complications, such as necrosis and gangrene, which can occur when the normal blood flow is not established in time. In addition, the necrotic tissue is more susceptible to become infected. Another complication is rhabdomyolysis, or muscle destruction, which ultimately leads to muscle scarring and contractures that restrict movement. Now, with rhabdomyolysis, myoglobin is released from the destroyed muscle cells into the bloodstream, and it’s filtered out by the kidneys. As a consequence, rhabdomyolysis can also result in acute kidney injury. Finally, acute compartment syndrome can result in irreversible nerve damage, leading to permanent motor and sensory deficits.
Now, when acute compartment syndrome is suspected based on history and physical exam, the next thing to do is to measure the compartment pressure using a handheld manometer. The diagnosis is confirmed if compartment pressure is greater than 30mmHg; or when the delta pressure, which is the diastolic pressure minus compartment pressure, is lower than 30mmHg. In addition, imaging techniques like X-rays, CT scan, MRI, and ultrasound can help locate bone, muscle, and blood vessel injuries. Laboratory tests are also done to monitor the client. These include a complete blood count showing elevated white blood cells, and an elevated erythrocyte sedimentation rate in case of infection. When rhabdomyolysis develops, a laboratory workup can show elevated levels of creatine kinase and myoglobin, while urinalysis can show tea colored urine due to high levels of myoglobin.
Acute compartment syndrome needs prompt action. When the compartment syndrome is caused by some external factors, like a cast, its removal can result in spontaneous recovery. Most often though, treatment involves a surgical procedure called fasciotomy, where the skin and fascia are cut open, relieving the pressure and reestablishing normal blood flow. However, if the tissue is already necrotic and gangrenous, the limb should be amputated.
All right, let’s begin Mr. Li’s assessment. After confirming his identity, you introduce yourself as his nurse and perform hand hygiene. Immediately, you notice Mr. Li is laying on the exam table grimacing in pain. You ask Mr. Li how he is feeling and he replies, “Terrible, I’ve never been in this much pain. And this feeling of pins and needles is driving me crazy! How can I make it go away?” On a scale of 0 to 10, he rates the pain in his right leg a 10.
Key Takeaways
Acute compartment syndrome is a condition that occurs when the pressure in a muscle compartment rises to a level that inhibits blood flow to the muscles and nerves. The main cause of this condition is blunt trauma, but it can also occur due to exercise-induced muscle damage, burns, or surgery. If left untreated, acute compartment syndrome can lead to permanent nerve damage and muscle ischemia, and eventually necrosis.
Sources
- "Diagnosing the Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition" Routledge (2019)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Elsevier (2022)
- "Critical care nursing: Diagnosis and management (9th ed)" Elsevier (2022)
- "Harrison’s principles of internal medicine" Mcgraw Hill (2022)
- "Acute compartment syndrome" Medicine (2019)
- "Diagnosing acute compartment syndrome—where have we got to?" International Orthopaedics (2019)
- "Acute compartment syndrome. Muscle, Ligaments and Tendons Journal" MLTJ (2015)