Antepartum assessment - Fetus: Nursing
Antepartum assessment - Fetus: Nursing
Acute Final
Acute Final
Notes
| ANTEPARTUM ASSESSMENT - FETUS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| FETAL MOVEMENT |
| |
| ULTRASOUND |
| |
| AMNIOCENTESIS & CHORIONIC VILLUS SAMPLING |
| |
| UMBILICAL ARTERY DOPPLER VELOCIMETRY |
| |
| NON-STRESS TEST |
| |
| CONTRACTION STRESS TEST |
| |
| BIOPHYSICAL PROFILE |
| |
Transcript
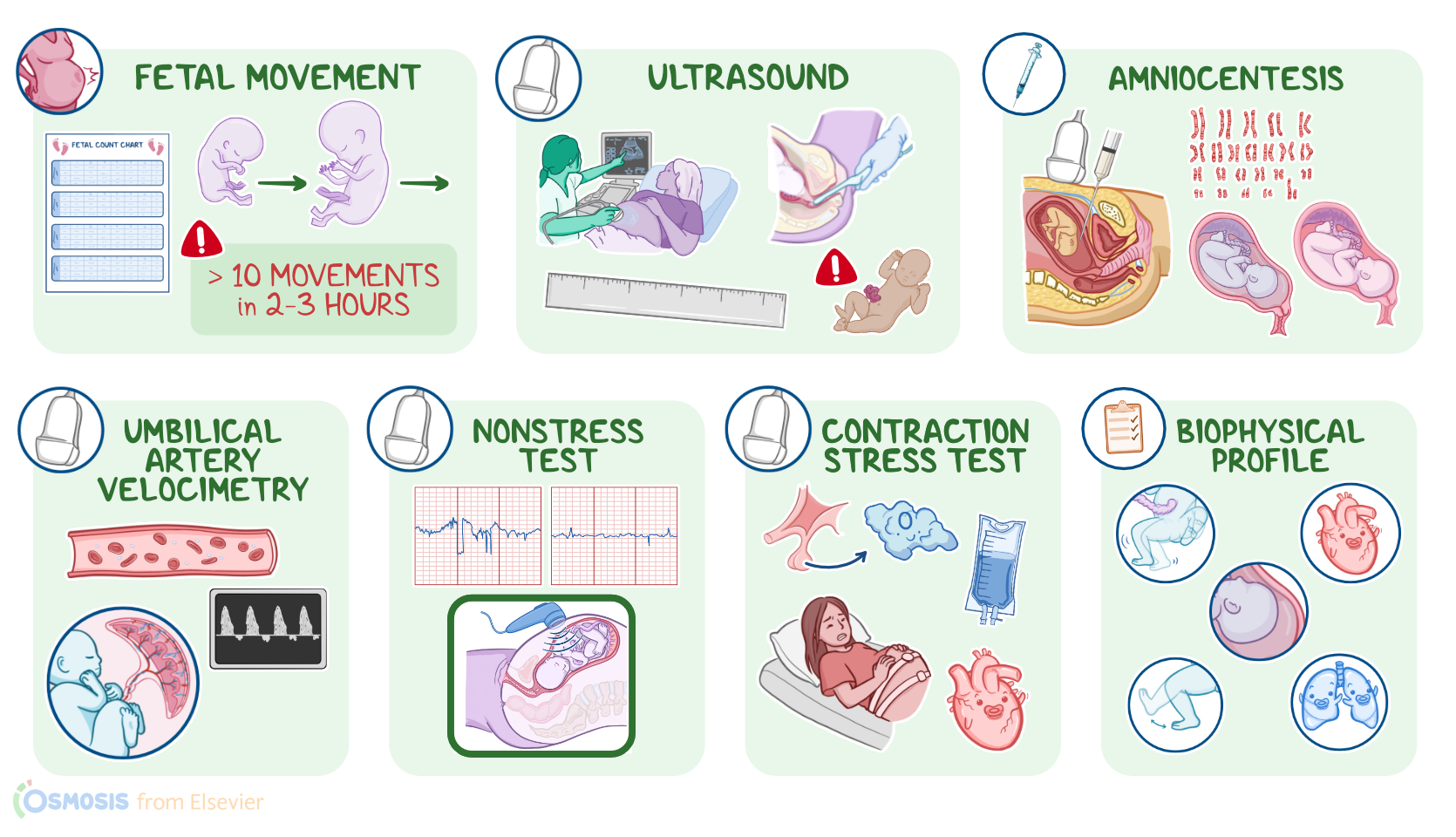
Antepartum fetal assessment refers to diagnostic procedures used to evaluate the fetal condition before birth.
Okay, let’s begin with assessment of fetal movement. Counting of fetal movements is a simple, cost-effective, and widely used method to monitor the well-being of a fetus. It’s based on the principle that if a fetus is compromised in some way, it will reduce its activity to conserve oxygen and energy. So, decreases in fetal movements or decreased activity in a previously active fetus might be due to a disturbance of placental function, and may precede an intrauterine fetal demise Now, fetal movements start around the 7th to 8th week of gestation, and increase as gestation progresses. These movements can be felt by the client, typically starting around the 16th and 18th weeks of gestation. One of the most common methods is the “count to ten” method. The client is instructed to count fetal movements, including at the same time each day, ideally this will be a time when the client knows her fetus will be active, which is often during the evening hours. Although there is no well-established evidence of the number of fetal movements that are considered normal, generally, if less than 10 movements in a 2-3 hour period are felt, the client should contact her healthcare provider.
Next up is ultrasound, which is a non-invasive test that uses high-frequency sound waves to visualize the fetus and monitor fetal growth; and can be done either transabdominally or transvaginally. Fetal growth can be assessed by measuring the biparietal diameter of the head and the fetal femur length, and birth weight can be estimated. Additionally, fetal anomalies such as open neural tube defects, including microcephaly or anencephaly, as well as ventral wall defects like omphalocele and gastroschisis can be detected. An ultrasound can also be used to measure nuchal translucency, which is a collection of fluid under the skin behind the fetal neck associated with trisomy 21.
Another important assessment is the amniotic fluid volume. Too much amniotic fluid, called polyhydramnios or sometimes hydramnios, is associated with problems that impair fetal swallowing, such as esophageal atresia. On the other hand, too little amniotic fluid, called oligohydramnios, is associated with uteroplacental insufficiency or problems that impair fetal urine production, including renal agenesis or polycystic kidneys.
Next, let’s look at amniocentesis, which is an invasive diagnostic procedure, where an ultrasound is used to guide a needle through the abdominal and uterine walls and into the amniotic sac. Once inside the amniotic sac, amniotic fluid is drawn, and analyses can be performed, including karyotyping, screening for congenital anomalies, and determining fetal lung maturity. An amniocentesis can also be used to remove excess amniotic fluid in cases of polyhydramnios.
On the other hand, there’s chorionic villus sampling, which involves taking a small sample of the placenta. A transabdominal approach is often used, where an ultrasound is used to locate the placenta, and a needle is inserted through the abdominal and uterine walls and into the placenta, where a sample is aspirated for chromosomal analysis.
Finally, it's important to note that these procedures can result in complications, including the risk of bleeding, infection, premature rupture of membranes, amniotic emboli, Rh isoimmunization, fetal injury, or spontaneous abortion.
Another technique is umbilical artery doppler velocimetry, which is a non-invasive method of evaluating blood flow in the maternal-fetal circulation, most often of the umbilical artery, using Doppler ultrasound. It assesses the direction of blood flow, as well as the velocity, volume, and resistance to flow from the fetus to the placenta. Common indications include pregnancies where uteroplacental insufficiency is suspected, like with preeclampsia, which causes placental resistance to increase.
Now, the Doppler captures the movement of red blood cells through the vessels, creating a waveform where the peak represents systole and the lowest represents diastole. When there is decreased, absent, or even backward blood flow during diastole, this is an indication that there’s high resistance in the placenta, which increases the risk of intrauterine growth restriction and fetal hypoxia.
Key Takeaways
Antepartum means before childbirth �. So, antepartum assessment refers to prenatal medical assessment of a mother and her fetus, aimed at assessing maternal and their health, diagnosing, managing, and counseling about any potential health issue. Antepartum assessment also includes assessing the fetus's size, measuring its head circumference and femur length, listening to its heart rate, and checking for any abnormalities on ultrasound or other various methods.