Arrhythmias - Asystole: Nursing
Notes
| ARRHYTHMIAS - ASYSTOLE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
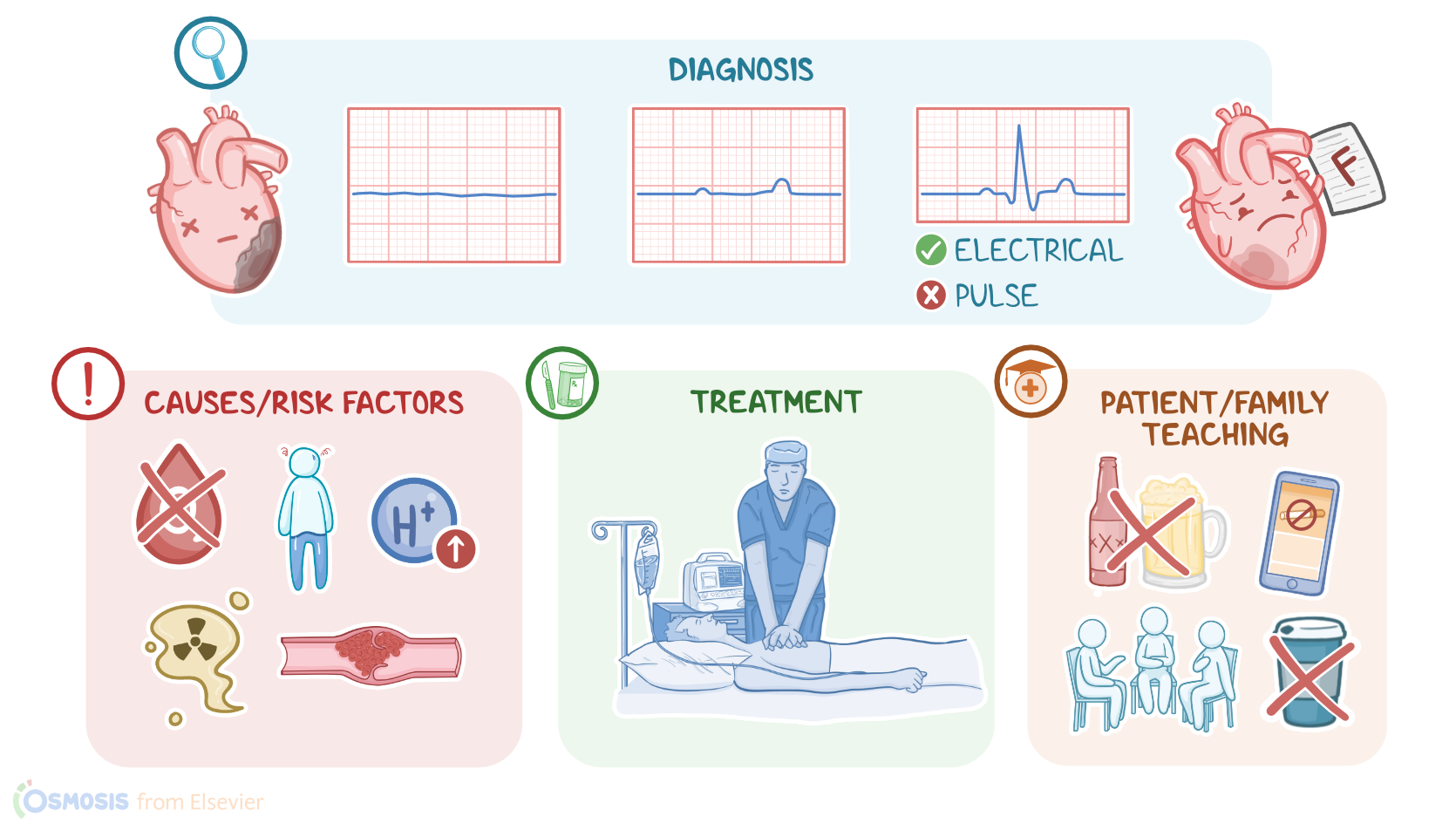
Cardiac arrest occurs when the heart suddenly stops pumping blood throughout the body. There are two types of cardiac arrest, asystole or cardiac flatline, and pulseless electrical activity, or PEA for short. Asystole is the most common type and refers to the total absence of electrical and mechanical activity of the heart. On the other hand, PEA occurs when there is electrical activity in the heart, but the cardiac muscle is unresponsive to stimulation; therefore, there’s no mechanical activity of the heart and pulse.
Now, let’s cover some physiology of the cardiac conduction system. The cardiac conduction system is made up of specialized myocardial cells that can create and transport electrical potential, also called an action potential. These cells have many special features, including automaticity, meaning that they can generate an impulse, excitability, which is the ability to respond to a stimulus by creating an electrical impulse, conductivity meaning they can carry the impulse to other cells, and contractility, which is the ability to shorten the length of their fibers, causing a contraction.
Alright now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atria , causing depolarization and creating the P wave on an ECG. When the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles.
From the atria, the impulse goes to the atrioventricular, or AV node, where the impulse propagation speed slows way down.
The interval from the atrial depolarization to just before ventricular depolarization is the PR interval on an ECG. This delay allows the atria to contract while the ventricles fill with blood.
From the AV node, the impulse goes through the Bundle of His, then to the right and left bundle branches, and finally through the Purkinje fibers, ...
which deliver the impulse to the right and left ventricles, causing them to depolarize,
and is represented by the QRS complex on an ECG. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations.
Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole.
And on ECG, ventricular repolarization will create a T wave, while the phase between ventricular depolarization and repolarization is represented by the ST segment.
Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Now, based on the cause, asystole can be classified as primary and secondary. Primary asystole occurs when the problem is at the level of the cardiac conduction system. On the other hand, secondary asystole occurs when some other condition that is not related to the cardiac conduction system affects the heart’s ability to fire and conduct electrical impulses. Secondary causes can be further subdivided into two main groups: 5 Hs and 5 Ts. 5 Hs include Hypoxia, or low levels of oxygen in peripheral tissues; Hypovolemia, or volume depletion; Hypothermia, or low body temperature; high concentration of Hydrogen ions, or acidosis; and finally, Hypo- or Hyperkalemia. On the flip side, 5 Ts include Toxins, cardiac Tamponade, Tension pneumothorax, pulmonary Thrombosis, and coronary Thrombosis.
Important risk factors associated with asystole include a medical history of cardiovascular conditions such as coronary artery disease and heart failure, as well as arrhythmias like ventricular fibrillation or V-fib, and ventricular tachycardia or V-tach. Additionally, advanced age, and chronic medical conditions such as kidney disease and diabetes mellitus can contribute to the risk.
Sources
- "Critical care nursing: Diagnosis and management (10th ed.) ISBN: 978-0-443-11581-3 " Elsevier (2026)
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 12th Edition. ISBN:978-0-323-78961-5 " Elsevier
- "Mosby’s® Diagnostic and Laboratory Test Reference. 15th edition. ISBN: 978-0-323-67519-2 " Mosby (2020)
- "Saunders Comprehensive Review for the NCLEX-RN. 9th Edition. ISBN: 978-0-323-79530-2 " Saunders (2022)
- "Fundamentals of Nursing. 11th edition. ISBN: 978-0-323-81034-0 " Elsevier (2022)
- "Seidel’s Guide to Physical Examination: An Interprofessional Approach. 10th edition. ISBN: 978-0-323-76183-3 " Elsevier (2022)
- "Critical Care Nursing: Diagnosis and Management. 9th edition. ISBN: 978-0-323-64295-8 " Elsevier (2021)
- "Invasive Management of Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Scientific Statement From the American Heart Association. 143(15):e815-e829." Circulation (2021)
- "Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. 143(21):e984-e1010." Circulation (2021)
- "Best Practices for Education and Training of Resuscitation Teams for In-Hospital Cardiac Arrest. 14(12):e008587." Circ Cardiovasc Qual Outcomes. (2021)