Arrhythmias - Ventricular fibrillation (Vfib): Nursing
Arrhythmias - Ventricular fibrillation (Vfib): Nursing
Perfusion
Perfusion
Notes
| ARRHYTHMIAS - VENTRICULAR FIBRILLATION (VFIB) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
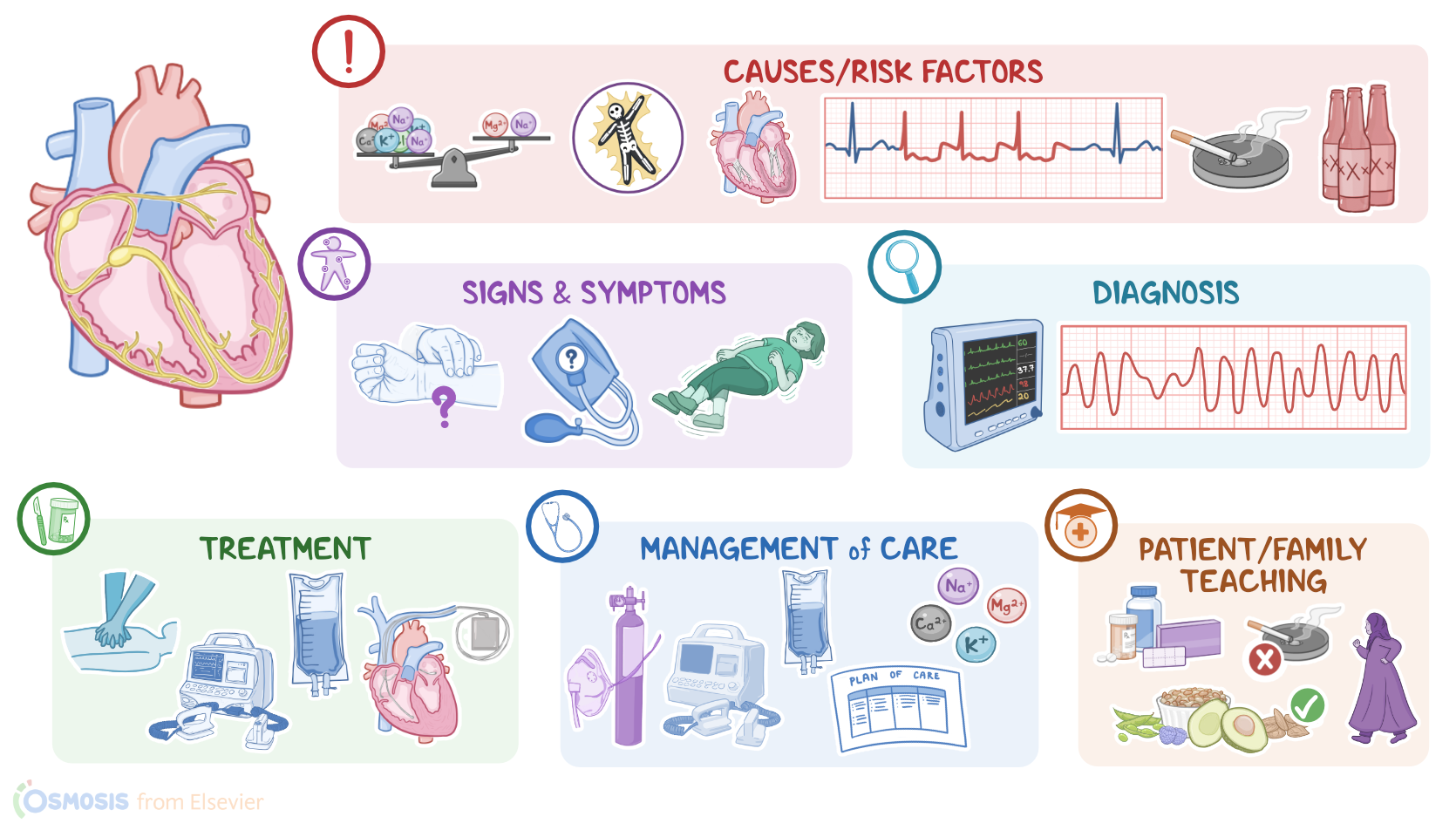
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILIY TEACHING |
| |
Transcript
Ventricular fibrillation or V-fib for short is a life-threatening condition, which occurs when the ventricular muscle fibers start firing impulses from multiple foci in a totally disorganized manner. As a result, instead of a single, coordinated contraction, there is quivering of the ventricles.
Now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atrium, creating the P wave on an ECG. And when the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles. From the atrium, electrical activity goes to the atrioventricular, or AV node, where the impulse propagation speed slows way down; this is the PR interval on an ECG. This pause allows the atria to contract while the ventricles fill with blood.
From the AV node, the depolarization wave goes through the Bundle of His, then the right and left branches of the Bundle, and finally through the Purkinje fibers, which deliver the current to the right and left ventricles, causing them to depolarize. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations, and it’s represented by the QRS complex on an ECG. Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the pause between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Okay, now back to ventricular fibrillation, which can be caused by disruption to normal heart muscle conductivity such as electrolyte imbalance, electrical shock, or certain illicit substances. Structural damage to the heart can also impair the heart muscle cells electrical properties.
These changes are strongly associated with several risk factors, including cardiovascular disorders. For example, myocardial infarction, and cardiomyopathies, and essentially anything that can create an inflammatory state or physically stretch out the ventricles, may potentially damage the cells in the ventricles and lead to ventricular fibrillation. Also, preexisting arrhythmias, like torsades de pointes and especially ventricular tachycardia, could become ventricular fibrillation. Other risk factors include a personal or family history of Brugada syndrome or ventricular fibrillation; stress, smoking, and excessive alcohol consumption.
When these risk factors lead to stress and damage to the ventricular muscle cells, it disrupts normal electrical conduction. When all the cells are homogenous, or the same, they all behave the same and can depolarize and contract in sync. On the other hand, damage causes areas with heterogenous cells which can conduct electrical impulses slower than others and are prone to abnormal behaviors like depolarizing on their own. So, when these heterogenous ventricular cells start randomly depolarizing out of sync with the rest of the heart, the impulses can spread to nearby cardiac tissue and ultimately circle back on itself and initiate another depolarization. This phenomenon is known as functional reentry and is thought to be the main mechanism that occurs in ventricular fibrillation. Because of this chaos, instead of having a single strong coordinated ventricular contraction, ventricular muscles begin to quiver, and start consuming a large amount of oxygen.
Now, the quivering ventricle can not generate enough force to pump out enough blood to meet the body’s demand. This situation is extremely dangerous, since the client’s body, especially the brain and the heart, isn't getting enough fresh oxygen, so ventricular fibrillation can lead to death within minutes of onset, which is called sudden cardiac death.
Clients with ventricular fibrillation typically present to the ER with a history of sudden collapse, unresponsiveness and periods of not breathing.