Aspergillosis: Nursing
Aspergillosis: Nursing
NRS 428 WK 2: Respiratory
NRS 428 WK 2: Respiratory
Notes
| ASPERGILLOSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
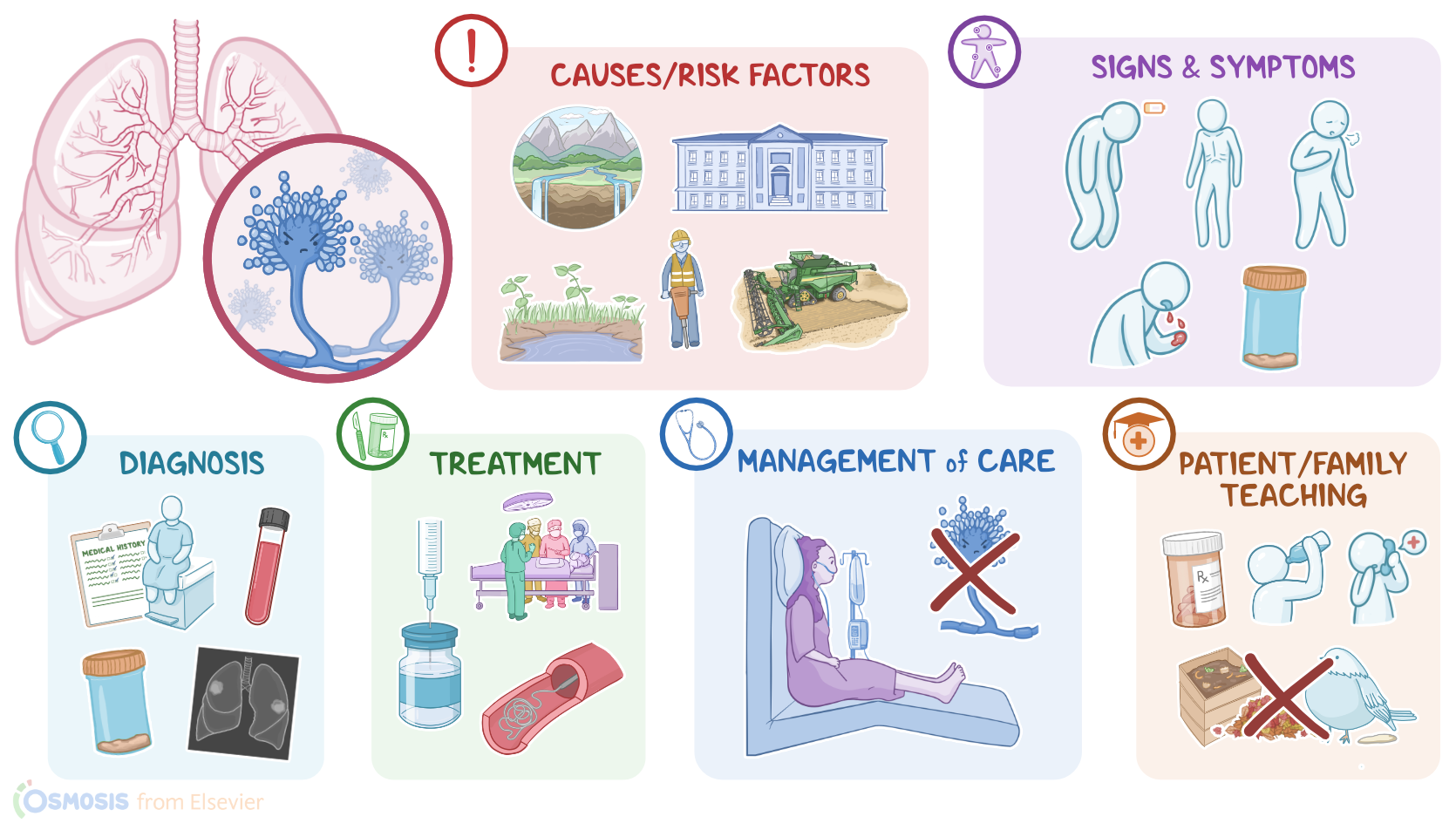
Aspergillosis is an infection caused by a fungus called Aspergillus, most commonly Aspergillus fumigatus, that typically affects the respiratory system. There are three types of aspergillosis; chronic, which is the most common; allergic; and invasive, which is the most severe.
Now, let’s quickly review the physiology of how the immune system fights off fungal infections. This is typically accomplished by white blood cells, which are part of the innate immune system. When a pathogen enters the body, the innate immune system reacts quickly. Some of the first cells on the scene include phagocytic cells like macrophages which essentially eat the pathogen. In response, they send out signals, such as beta-d-glucan, to activate other cells like neutrophils to surround and kill the pathogen. These combined, non-specific innate immune responses kill most fungal pathogens before they can spread around the body.
Now, the cause of aspergillosis is being exposed to the Aspergillus fungus. This fungus is ubiquitous, and particularly loves damp areas, older buildings, moist soil, and damp woods and leaves, so working in construction or farm jobs in these areas puts a client at higher risk for developing an Aspergillus infection.
Additionally, risk factors for severe aspergillosis include being immunocompromised because of AIDS or neutropenia; long-term term steroid use; or anti-rejection medications after a transplant. Also, chronic lung disease like COPD, asthma, TB, and cystic fibrosis put clients at increased risk.
Okay, now, the pathology of aspergillosis typically begins when a person inhales Aspergillus spores which then land in the respiratory tract, particularly the lungs. If the client’s immune system doesn’t properly clear the infection, then the spores are able to grow into fungi and spread throughout the lungs. When clients are severely immunocompromised, the infection can spread to the brain, heart, kidneys, or skin at which point it is considered invasive aspergillosis. This is a potentially life-threatening scenario. Alternatively, the fungal spores in the lung cavity may grow into a ball of fungus called an aspergilloma. The infection can also cause complications like lung fibrosis, respiratory failure, CNS infection, and endocarditis.
Typically, the clinical manifestations of aspergillosis include fatigue, malaise, weight loss, and fever, as well as shortness of breath, hemoptysis, production of brown sputum containing fungus plugs, as well as pulmonary rales on auscultation. Sinus tenderness and epistaxis can also be present if the fungus has invaded the sinuses. Aspergillosis can spread to other parts of the body like the eyes, causing periorbital cellulitis, to the central nervous system resulting in altered mental status and even seizures.
Diagnosis of aspergillosis begins with the client’s history and physical assessment. A sputum culture can show fungal hyphae in the sputum, while a blood sample can identify biomarkers for aspergillosis like galactomannan and beta-D-glucan. If the client has a chronic infection, IgG antibodies against Aspergillus can be present in the blood. Additionally, a biopsy or bronchoscopy can help the diagnosis. Finally, to identify aspergillomas, cavitations, or lung fibrosis, a chest X-ray or CT can be performed.
Treatment of aspergillosis includes supportive care and long-term antifungal medications for about six months that are initially given intravenously. For severe infections, surgery can be necessary to remove pulmonary aspergillomas, and for allergic aspergillosis, corticosteroids are typically given. Lastly, for severe hemoptysis, an embolization procedure can be performed to occlude the blood vessels that are leaking into the lungs.
All right, let’s look at the nursing care you’ll be providing for a client with aspergillosis. Your priority nursing goals are to eliminate the infection and promote adequate ventilation and oxygenation.