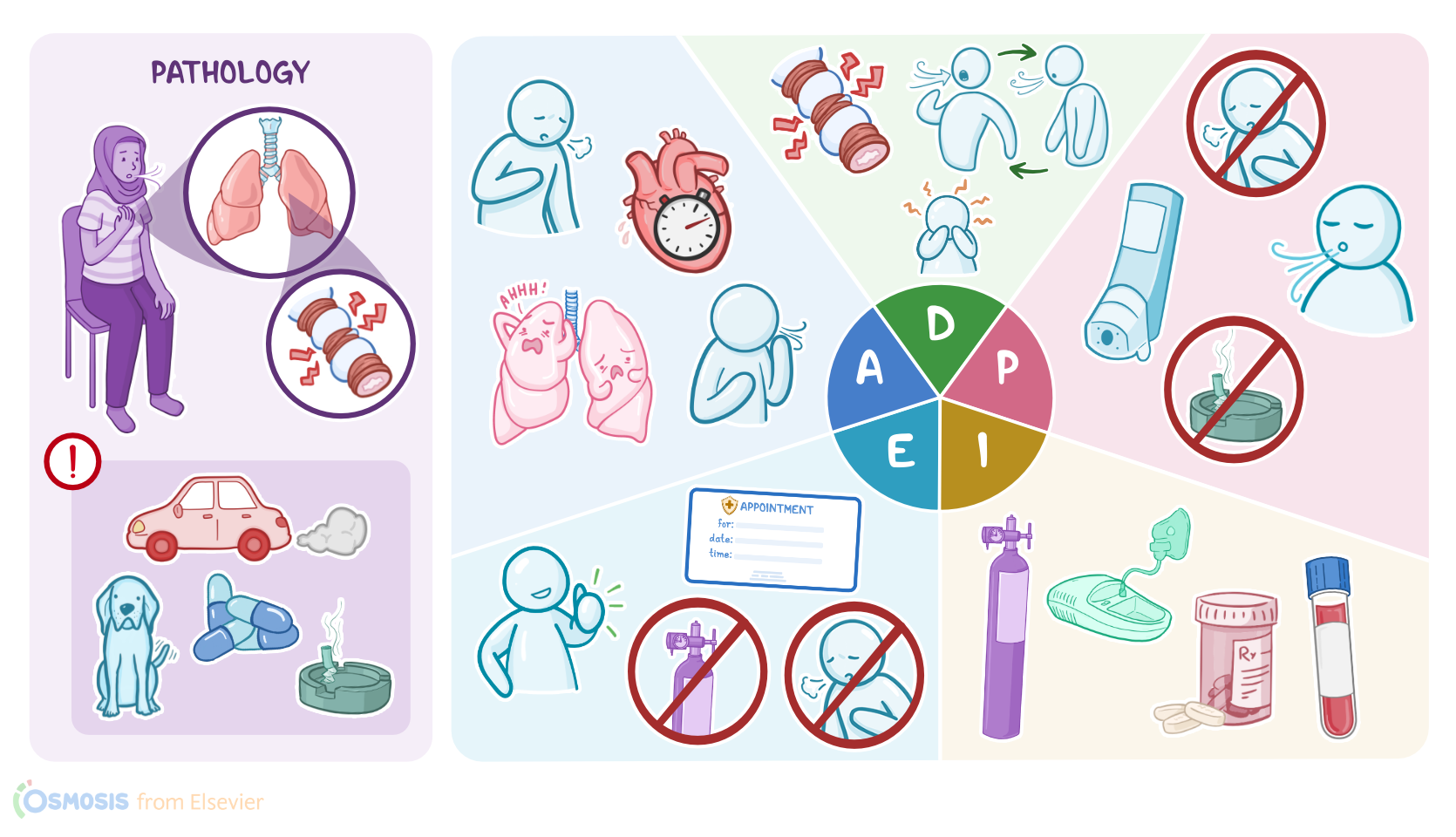
Asthma: Nursing process (ADPIE)
2,850views
Asthma: Nursing process (ADPIE)
medsurg 2
medsurg 2
Notes
| ASTHMA | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Megan Fitzpatrick is a 29-year-old woman with a history of asthma who was brought to the emergency department, or ED, by a friend after having trouble breathing which was not resolved with the use of her inhaler. Megan presents with wheezing, shortness of breath, and chest tightness. She is able to speak in short sentences but frequently pauses to breathe. She appears anxious and states her asthma has never felt this awful before.
Asthma is a chronic inflammatory disease of the airways characterized by bronchial hyperresponsiveness and airflow obstruction. Although the specific causes of asthma are ultimately unknown, it’s thought to be caused by a combination of genetic and environmental factors.
Asthma symptoms are often initiated by an environmental trigger. The triggering substance can differ from person to person, but some common ones include air pollution, like cigarette smoke and car exhaust, as well as allergens like dust, pet dander, cockroaches, and mold. Medications like aspirin and beta-blockers have also been known to trigger symptoms in some individuals with asthma. Lastly, cold, dry air or exercise can also trigger asthma in some individuals.
Inhaling a triggering substance can initiate what is known as an asthma exacerbation or attack. The triggering substance travels down the airways to the bronchioles, which are composed of cartilage, smooth muscle, and a mucosal lining containing mucus-secreting goblet cells. Immune cells such as mast cells and basophils, are stimulated to release chemical mediators such as histamine and leukotrienes that cause the smooth muscle in the bronchioles to spasm, known as a bronchospasm, and cause the goblet cells to produce an abundance of mucus.
Together, bronchospasm and mucus obstruct the airway, making it difficult to breathe, and leading to symptoms such as coughing, chest tightness, dyspnea, and wheezing, which is a high-pitched whistling sound that usually happens during exhalation. Over time, chronic inflammation can lead to scarring and fibrosis which can permanently reduce the airway diameter.
When asthma is initially suspected, the first step in diagnosis is conducting pulmonary function tests, or PFTs. The most important measurements are the forced vital capacity, or FVC and forced expiratory volume at 1 second, or FEV1. FVC is is the total volume of gas exhaled after forced full inspiration, whereas FEV1 refers to the forced expiratory volume at 1 second. Both the FVC and FEV1 are decreased in asthma. A FEV1/FVC ratio less than 70 percent indicates airway obstruction.
In an emergency situation, the quickest way to measure airway obstruction is measuring the peak expiratory flow rate, or PEFR, which is essentially the fastest and the hardest a person can exhale after a full inspiration. PEFR is kind of like a bedside mini-PFT; not quite as reliable, but very useful in an emergency setting. A normal PEFR is greater than 70 percent of the predicted peak flow for the client’s age.
While there is no cure for asthma, there are treatments that can help manage the symptoms. It begins with avoiding or minimizing contact with triggering substances. Then, depending on the frequency and severity of the symptoms, a stepwise and individualized pharmacological approach is used to control symptoms and prevent exacerbations.
Medications used for asthma management include bronchodilators that cause smooth muscles in the lungs to relax such as inhaled short-acting beta-agonists like albuterol, long-acting beta-agonists like formoterol, or anticholinergics like ipratropium. Corticosteroids like inhaled budesonide or oral prednisone reduce airway inflammation and mucus secretion.
Leukotriene receptor antagonists, or LTRAs like montelukast, block the production of leukotrienes. Mast cell stabilizers, like cromolyn, prevent the release of inflammatory chemicals from mast cells. And finally a monoclonal antibody called omalizumab lowers IgE levels, which then decreases the release of chemical mediators from immune cells.
In the event of a severe asthma exacerbation that does not resolve with the prescribed medication regimen, a visit to the ED is needed. Once there, additional tests will determine the severity of the attack and appropriate treatment. An arterial blood gas, or ABG, may initially show respiratory alkalosis due to hyperventilation; however, as symptoms progress, respiratory acidosis, a sign of impending respiratory failure, may develop.
Increased eosinophils are often evident on a complete blood count, or CBC. Treatment during an asthma exacerbation will immediately begin with a bronchodilator and supplemental oxygen titrated to an oxygen saturation above 92 percent. Other medications will be administered until the exacerbation resolves.
Okay, let’s get back to our client Megan. After presenting in the ED, Megan is triaged quickly for a severe exacerbation of asthma. She receives a dose of albuterol via nebulizer, is started on 2L of oxygen via nasal cannula with continuous pulse oximetry, and moved to an ED bed for further management. After entering her room, you introduce yourself, wash your hands, and confirm her identity.
Upon visual inspection, Megan is sitting upright and appears to be in respiratory distress. She states she woke up this morning with increased shortness of breath, coughing, and chest tightness. After using her inhaler three times with no relief, she asked her friend to drop her off at the ED. You auscultate her lungs which reveals a bilateral expiratory wheeze and diminished breath sounds. You note visible intercostal and substernal retractions while she is breathing. Her heart rate is regular but tachycardic. She denies chest pain but states her chest feels tight. Capillary refill is less than 3 seconds.
Sources
- "Severe asthma in children: Evaluation and management. " Allergol Int. (2019;68(2):150-157. )
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care. 13th edition. ISBN: 978-0-323-77683-7 " Mosby (2022)
- "The basic immunology of asthma [published correction appears in Cell. 2021 Apr 29;184(9):2521-2522]. " Cell (2021;184(6):1469-1485. )
- "Critical Care Nursing: Diagnosis and Management. 9th edition.ISBN: 978-0-323-64295-8 " Elsevier (2021)
- "Harrison’s Principles of Internal Medicine. 21st edition. ISBN: 978-1-264-26850-4 " McGraw Hill / Medical (2022)
- "Genetics and Epigenetics in Asthma. " Int J Mol Sci. (2021;22(5):2412. Published 2021 Feb 27. )