Bone tumors: Nursing
Notes
| BONE TUMORS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
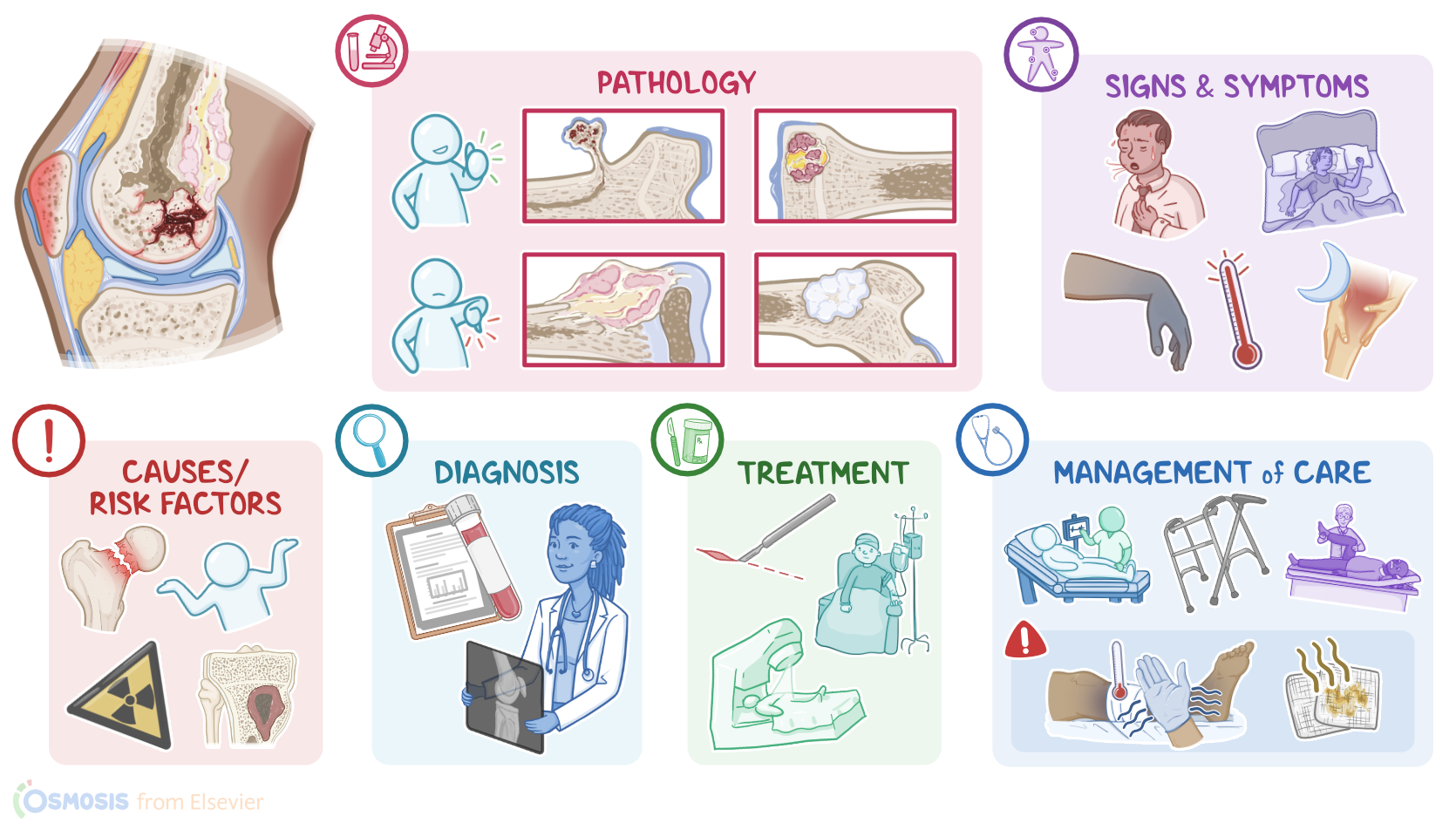
Bone tumors are abnormal growths in the bone that can be broadly classified into benign and malignant. Benign bone tumors stay localized to the bone, and include osteochondroma, giant cell tumor of bone, osteoblastoma, osteoid osteoma, and enchondroma.
In contrast, malignant bone tumors can spread to surrounding tissues and organs. They are further classified as primary malignant tumors, which originate from bone cells, and include osteosarcoma, chondrosarcoma, and Ewing sarcoma; and secondary or metastatic tumors, which originate from other sites in the body, most commonly breast, lung, or prostate; and travel to the bones via lymphatic or blood vessels.
Okay, let’s start by looking at the physiology and anatomy of the bones. Normally, the bones’ surface is covered by a dense layer of connective tissue called the periosteum, and it's where the muscles, tendons, and ligaments are attached. Beneath the periosteum, there’s a dense external layer called compact bone; and a softer internal layer called spongy or trabecular bone, which normally consists of trabeculae and pores resembling a honeycomb.
Now, looking at a long bone, like the femur, it has two epiphyses, which are at the ends that contribute to joints with other bones and are mostly made up of trabecular bone. Between the two epiphyses, is the diaphysis or bone shaft, made up mostly of cortical bone, and a central hollow space, known as the medullary cavity. Bone marrow occupies both the medullary cavity and the spaces in the spongy bone of the epiphysis, which is the site of blood cell production.
Now, in children and adolescents, there’s an additional narrow portion between the epiphysis and the diaphysis called the metaphysis, which is mostly made of trabecular bone. The metaphysis contains the growth plate, a cartilaginous tissue that actively grows during childhood. By adulthood, the growth plate has ossified and fused with the diaphysis and the epiphysis, becoming a mature bone.
Now, all bones are basically made of the same types of cells, chief among them are osteoblasts, which build up new bone, and osteoclasts, which help with bone breakdown or resorption. In addition to these, there are some more primitive cells in the bone marrow called human mesenchymal stem cells and neuroectodermal cells, which have the ability to differentiate into many cell types including nerve, fat, bone, and cartilage cells.
Now, the exact cause of bone tumors is unknown, but they are thought to occur when bone cells acquire mutations that let them grow and divide out of control. Typically these are mutations in proto-oncogenes, which promote cell division, or mutations in tumor suppressor genes, which result in a loss of inhibition of cell division.
Now, mutations may arise due to a variety of risk factors. Risk factors for all bone tumors include bone trauma, chronic osteomyelitis, and exposure to radiation.
Osteosarcoma, specifically, occurs most commonly in clients who are assigned male at birth, and are between 10 to 25 years of age. It is not as prevalent in older clients, where it usually develops secondary to predisposing factors, like Paget disease of bone, which is a condition where there’s abnormal bone remodeling; bone infarcts; familial retinoblastoma which is a childhood malignant tumor of the eye; and Li-Fraumeni syndrome, a condition that predisposes to a variety of cancers throughout the body.
In contrast, chondrosarcoma tends to affect adult clients between 50 to 70 years of age, while Ewing sarcoma is more common in children and teenagers.
Okay, so the pathology of bone tumors begins once a cell becomes mutated and starts dividing uncontrollably, forming a tumor.
The most common type of benign bone tumor is osteochondroma, which is thought to arise from the growth plate, and it typically results in a lateral bony projection. This bony stalk is called an exostosis, and it has a cap, made mostly of hyaline cartilage.
Osteochondromas typically develop in the metaphysis of long bones, most commonly the distal femur and the proximal tibia, around the knee joint, but they can also occur in flat bones like the ilium, one of the hip bones, as well as the scapula.
Another benign bone tumor is the giant cell tumor of the bone, which contains giant osteoclast-like cells with numerous nuclei, and develops in the epiphysis of the long bones, like the distal femur and the proximal tibia.
Next are osteoblastomas, and osteoid osteomas, both of which arise from osteoblasts. Osteoblastomas also tend to affect the bones of the axial skeleton, usually the mandible, whereas osteoid osteomas typically affect the diaphysis of long bones like the tibia.
Finally, enchondromas arise from cells called chondrocytes, which produce cartilage, and typically develop in small bones of the hands and feet.
Now, among malignant tumors, the most common one is osteosarcoma, which arises from osteoblasts and often forms in the metaphysis of long bones, especially in the knee region.
Chondrosarcoma arises from mutated chondrocytes, and mainly affects the medullary cavity of the bones of the pelvis, but can also affect long bones, like the humerus and proximal femur.
Finally, Ewing sarcoma is thought to arise from neuroectodermal cells and tends to grow in the diaphysis of long bones like the femur, as well as in pelvic flat bones.
Now, both benign or malignant tumors can grow in size, and compress or destruct nearby structures, or cause a reactive osteoclast response, which leads to bone resorption. Eventually, a malignant tumor can spread to nearby tissues or get into the bloodstream and metastasize to other parts of the body, especially to the lungs.
Now, the clinical manifestations of bone tumors differ based on their size and location. In general, bone tumors may cause bone pain, swelling due to the tumor growing in size, as well as pathologic fractures.
In terms of unique symptoms, osteoid osteoma is characterized by pain that typically gets worse at night; while osteochondromas and osteoblastomas sometimes press against spinal nerves, causing numbness and limb weakness. Clients with malignant bone tumors, especially Ewing sarcoma, often experience fever, night sweats, and weight loss. If the bone tumor metastasizes to the lungs, clients can also present pulmonary symptoms like coughing and shortness of breath.
Diagnosis of bone tumors begins with the client’s history and physical assessment. Lab findings can also be helpful and usually show increased serum alkaline phosphatase or ALP in malignant tumors, plus anemia, leukocytosis, and increased serum lactate dehydrogenase or LDH in Ewing sarcoma. Elevated serum calcium and erythrocyte sedimentation rate or ESR can also be present in metastatic disease.