Bronchopulmonary dysplasia (BPD): Nursing
Notes
| BRONCHOPULMONARY DYSPLASIA (BPD) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Bronchopulmonary dysplasia, or BPD, also known as neonatal chronic lung disease, is an iatrogenic respiratory disease most commonly affecting preterm newborns that results from lung injury and disrupted lung development.
Now, let’s quickly review the respiratory tract, which can be divided into two regions: the upper respiratory tract and lower respiratory tract. The upper respiratory tract includes the nose, nasal cavity, the oral cavity, pharynx, epiglottis, larynx, and the upper part of the trachea; while the lower respiratory tract includes the lower part of the trachea, and the lungs containing the bronchi. These are lined by pseudostratified ciliated columnar epithelium. This contains goblet cells, which produce mucus to trap small foreign particles; as well as columnar cells, which have cilia, or tiny little hair-like projections that move mucus and foreign particles up the respiratory tract. The bronchi gradually branch into bronchioles, which give rise to the alveolar ducts, and finally the alveoli. Alveoli are tiny air-filled sacs that are surrounded by tiny blood vessels, called capillaries.
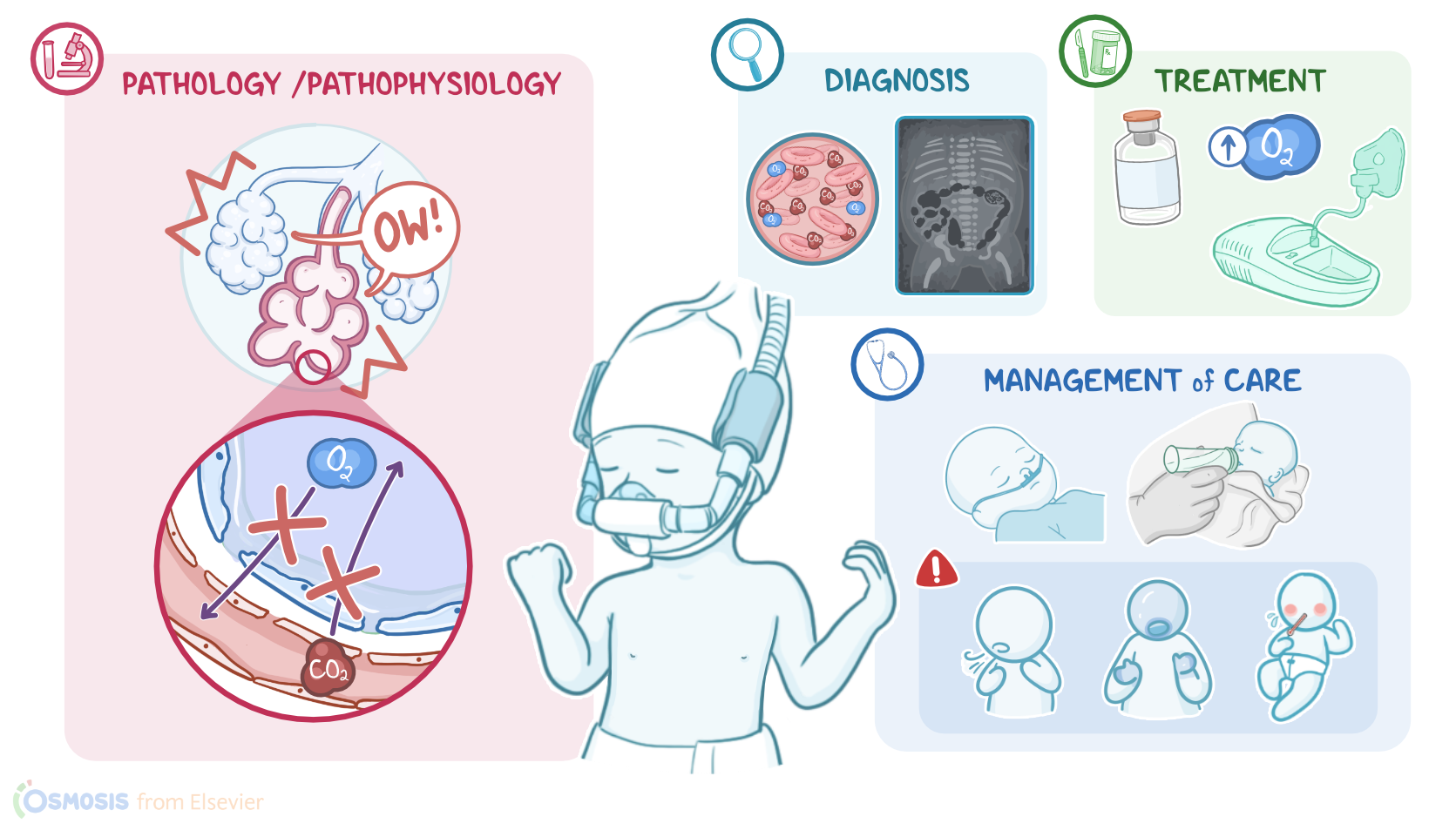
If we zoom in even more, we can see a tiny space between the alveolar wall and the capillary wall, called the interstitial space. And that’s where most gas exchange occurs, so as we breathe, the inhaled oxygen moves through the alveolar membrane, the interstitial space, and the capillary membrane to reach the blood, while the carbon dioxide moves from the capillaries through the interstitial space and into the alveolar sacs to be exhaled. Now, the alveoli are lined by alveolar epithelial cells, called pneumocytes. The vast majority are type I pneumocytes, which allow oxygen and carbon dioxide to pass through them. There are also type II pneumocytes scattered around which produce surfactant, an oily secretion that coats the alveoli and prevents their collapse.
Alright, now the cause of BPD is multifactorial, and is often due to positive pressure ventilation. This can cause barotrauma due to high airway pressure, volutrauma where alveoli become overdistended, and the production of reactive oxygen species from high inspired oxygen concentrations. The lungs are also at higher risk of being damaged if there’s abnormal lung growth and impaired alveolar development which results in fewer and larger alveoli.
So, the most important risk factors for developing BPD include prolonged mechanical ventilation and oxygen supplementation. BPD is particularly common in preterm infants, especially those born before 32 weeks of gestation, as well as infants with low birth weight, and those with intrauterine growth restriction or IUGR for short. Additionally, patent ductus arteriosus, intrauterine and postnatal infections, and maternal smoking may increase the risk for BPD.
Okay, regardless of the risk factor, the pathology of BPD involves lung injury. When the lungs are injured, immune cells start producing pro-inflammatory cytokines which trigger inflammation, edema and fibrosis of the interstitial space, inhibiting gas exchange even more. Inflammation also causes capillaries to become permeable to larger molecules like proteins, which leak into the alveoli, pulling interstitial fluid with them. The end result is noncardiogenic pulmonary edema. Meanwhile, damaged type II pneumocytes stop producing surfactant, causing alveolar collapse. These collapsed, fluid-filled alveoli cannot participate in gas exchange. This results in hypoxemia, or low oxygen in the blood, and hypercapnia or high carbon dioxide in the blood. The inability to get rid of carbon dioxide results in respiratory acidosis.
At the same time, lung injury can cause decreased alveolar capillary formation. Fewer alveolar capillaries causes increased pulmonary resistance, which can ultimately lead to pulmonary hypertension.
Lastly, the bronchi may become hyper-reactive to stimuli and secrete more mucus while losing their cilia which makes it easier for foreign particles to reach the lungs.
Complications of BPD include right ventricular hypertrophy, which can ultimately lead to heart failure. Other complications include subglottic stenosis, or narrowing of the airway below the vocal cords, tracheobronchomalacia, where the tracheal and bronchial walls are floppy, and prone to collapse, as well as bronchospasms, and aspiration of gastric fluids.
Finally, long-term outcomes of infants with BPD include increased risk of developing bacterial and viral infections, persistent abnormalities in pulmonary function, sleep hypoxemia, neurodevelopmental delay, and growth impairment.
Clinical manifestations of bronchopulmonary dysplasia include continued dependence on oxygen and positive pressure ventilation. Other findings include increased respiratory secretions, nasal flaring, tachypnea, tachycardia and intercostal or substernal retractions during inspiration, along with grunting during expiration, as well as intolerance to handling and feeding.
During auscultation of the chest, there are typically decreased breath sounds, as well as diffuse crackles which is the sound of collapsed alveoli popping open with inspiration. Intermittent expiratory wheezing might be also audible.
Diagnosis of BPD starts with the client’s history and physical assessment. More specifically, it is based on the need for oxygen supplementation for at least 28 days postnatally, and it’s graded as mild, moderate, or severe. Additionally, arterial blood gas analysis can show hypoxemia, hypercapnia and respiratory acidosis. Finally, a chest radiograph is recommended to assess the extent of the disease, and can reveal diffuse haziness, due to the fluid accumulation, as well as peribronchial thickening and hyperinflation.
Treatment of BPD is mainly supportive to decrease the work of breathing to allow for optimal growth and development. It involves respiratory support and supplemental oxygen with gradual weaning, when possible. Surfactant supplementation can promote better ventilation and pressure distribution in the alveoli during mechanical ventilation, preventing overdistention, decreasing inflammation, and stabilizing the alveoli. Inhaled bronchodilators can be used to reduce airway resistance, and in severe cases, inhaled corticosteroids, might also be needed to reduce inflammation.
Additionally, nutritional support, with increased caloric and protein intake, and fluid restriction, are important. Those who do not respond or cannot tolerate fluid restriction may require diuretics. Antibiotics should also be administered in the case of bacterial infection. Finally, incidence and severity of BPD can be reduced with prevention of preterm birth, administration of antenatal steroids, administration of methylxanthines like caffeine, and vitamin A; and early weaning from positive pressure ventilation.