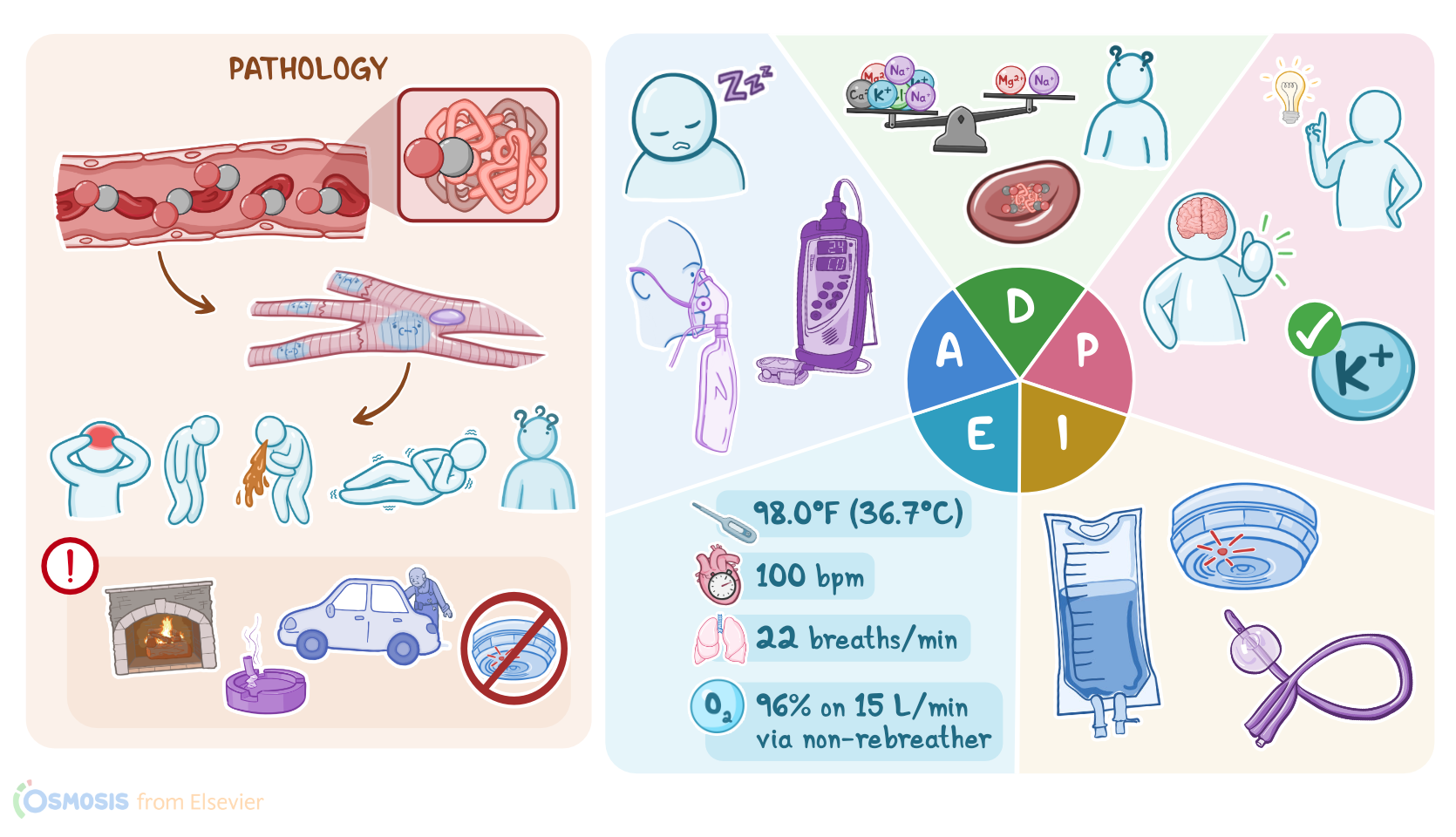
Carbon monoxide poisoning: Nursing process (ADPIE)
Carbon monoxide poisoning: Nursing process (ADPIE)
Critical Care - Nursing
Critical Care - Nursing
Notes
| CARBON MONOXIDE POISONING | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Emma Rogers is a 12-year-old female brought to the ED by paramedics. Emma’s mother Faye called emergency services when she went to Emma’s room to wake her up and noticed she was lethargic, confused and unable to stay awake. The paramedics found Emma in her basement bedroom which was adjacent to a hot water heater. Carbon monoxide poisoning is suspected.
Carbon monoxide poisoning occurs when there’s a buildup of carbon monoxide in the blood. CO is produced from the burning of fuels that contain carbon, such as charcoal, oil, coal, wood and kerosene. It is known as the “silent killer” because it’s odorless, tasteless, and colorless.
Some classic scenarios where CO poisoning can occur include: an individual that’s been in a fire and has inhaled smoke; someone in a poorly ventilated area with a running vehicle, fireplace, or faulty gas stove or hot water heater; or if they live in an old building with a defective heating system. An individual may also be chronically exposed to CO, and that’s common in smokers, automobile workers, and people working in certain industries.
Now, there are some factors that may put an individual at risk for CO poisoning. Non-modifiable risks include age, in particular young children and the elderly, as well as those with physical or mental disabilities.
These factors can make it harder for the individual to stop or escape from the situation where CO is being produced. In addition, cigarette smoking and having an underlying lung disorder increases the risk of harm from CO poisoning.
On the other hand, modifiable risk factors include being in a building without functioning CO detectors, or being under the influence of alcohol or drugs.
Now, once CO is inhaled, it makes its way into the bloodstream. The affinity of hemoglobin for CO is about 240 times more than its affinity for oxygen, so CO will competitively bind to hemoglobin, forming carboxyhemoglobin, or COHb, and the oxygen carrying capacity of blood decreases.
Also, the presence of CO in the blood makes it difficult for oxygen to be released into the tissue. Ultimately, the combination of decreased oxygen carrying capacity and impaired unloading ultimately leads to tissue hypoxia and injury.
Now, the signs and symptoms associated with CO poisoning can vary and depend on the duration of CO exposure, and the amount of carboxyhemoglobin in the blood.
In acute cases, the most common symptoms include a headache, fatigue and dizziness. Some clients may also develop abdominal pain, nausea and vomiting. As poisoning progresses, they can have confusion, and difficulty concentrating. Other frequent symptoms are dyspnea, palpitations and seizures.
If the client is found after hours of being exposed to CO, their skin and mucosal surfaces may have a characteristic pink or cherry red discoloration. They may also have bullae, blisters, and other erythematous spots on skin. Chronic poisoning is usually more insidious and can easily be mistaken for flu or gastroenteritis.
Clients with CO poisoning often develop complications. Hypoxia can lead to metabolic acidosis, myocardial infarction, as well as rhabdomyolysis, or skeletal muscle destruction, which can lead to acute renal failure.
Severe tissue hypoxia can also lead to brain edema, pulmonary edema, and eventually respiratory failure, cardiac arrest, coma, and even death. Fortunately, most clients who survive CO poisoning don’t develop long term complications.
However, some important ones to keep in mind include delayed neurological sequelae like cognitive deficits, personality changes, movement disorders like tremors or paralysis, and focal neurological deficits like numbness of the fingers and toes. These deficits can last for a year or longer.
If the client’s history and symptoms suggest CO poisoning then a CO-oximeter should be used to detect the level of carboxyhemoglobin. Regular pulse oximetry can’t differentiate between oxyhemoglobin and carboxyhemoglobin so the reading will typically be normal.
Next, arterial blood gas analysis typically shows decreased oxygen saturation and elevated carboxyhemoglobin levels, while partial pressure of oxygen remains normal. If the client has chest pain, an ECG should also be done as soon as possible to look for ischemic changes, like ST depression or ST elevation.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Carbon Monoxide Poisoning" Crit Care Clin (2021)
- "Emerging cellular-based therapies in carbon monoxide poisoning" Am J Physiol Cell Physiol (2021)
- "Carbon monoxide poisoning" Toxicol Rep (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Neurocognitive sequelae after carbon monoxide poisoning and hyperbaric oxygen therapy" Med Gas Res (2020)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Carbon monoxide poisoning" Undersea Hyperb Med (2020)