Cesarean birth: Nursing
Notes
| CESAREAN BIRTH | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
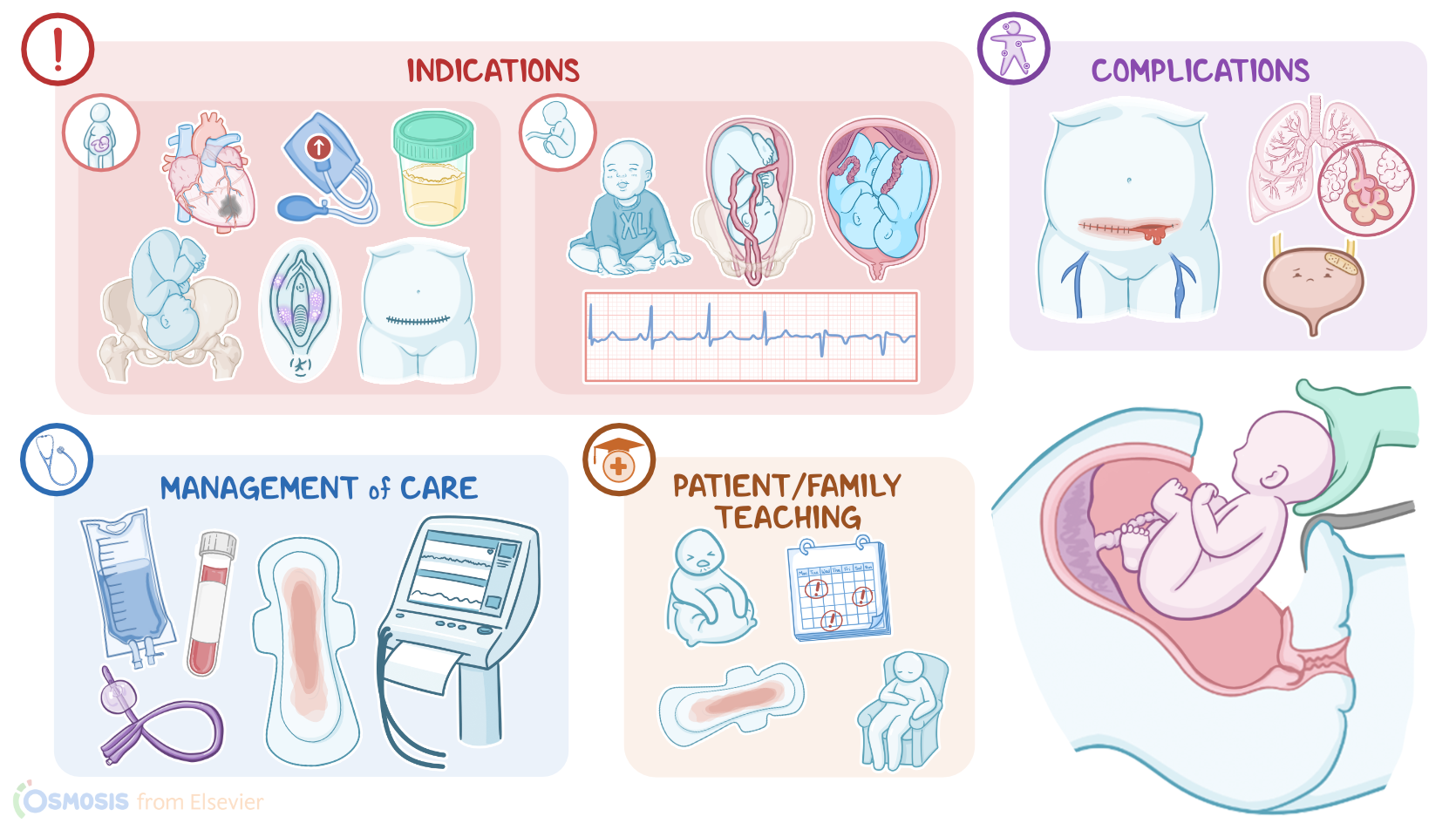
| INDICATIONS |
| |
| PROCESS |
| |
| COMPLICATIONS |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Cesarean birth is when the fetus is delivered through a surgical incision in the abdominal wall and the uterus.This type of delivery is preferred if a vaginal delivery could compromise the fetus, the mother, or both; or if the delivery of the fetus needs to be accomplished urgently. Other times, a cesarean delivery can also be performed on maternal request. Maternal indications can include heart disease; preeclampsia, which is when hypertension is associated with proteinuria; placental problems such as placenta previa or placental abruption; cephalopelvic disproportion, where the maternal pelvis is too small for the fetal head to pass through; active genital herpes simplex virus infection that can be transmitted to the fetus during vaginal birth; and previous uterine surgeries, such as previous cesarean birth due to risk of uterine rupture at the scar site. Fetal indications can include abnormal fetal heart rate tracings; malpresentation, such as breech or transverse lie; prolapsed umbilical cord; as well as congenital malformations or intrauterine infections. Some other fetal-related risk factors include fetal macrosomia, and multiple gestation, such as twin pregnancies.
Let’s switch gears now and go through the process of cesarean birth. The first step is preparation of the client for the procedure. This includes routine preoperative laboratory tests, such as complete blood count, blood typing and screening; continuous fetal monitoring; and administration of prophylactic antibiotics. A wedge is placed under one hip to reduce uterine compression of the aorta and inferior vena cava, and to promote placental blood flow. A urinary catheter is placed to help empty the bladder. Then, the anesthesiologist administers regional anesthesia, like an epidural, or combined spinal-epidural anesthesia. If cesarean birth is performed as an emergency procedure, then general anesthesia can be chosen as it can be administered much quicker. Lastly, sterile abdominal skin preparation is done, cleaning it with a solution like povidone iodine and applying it in a spiral motion away from the umbilicus or away from the incision site.
Now, after the client is prepared for the procedure, the next step involves making an incision in the abdominal wall, starting with the skin. The most common skin incision is a low transverse incision just above the symphysis, which leaves a smaller scar and lowers the chance of dehiscence or hernia formation. The other type of skin incision is midline vertical incision between the umbilicus and symphysis, which is usually more suitable for clients with abdominal obesity. This incision can be done much faster, provides better visualization of the uterus and can easily be extended superiorly if needed. After the abdominal wall is opened, the bladder is separated from the uterus using a retractor. Then, a second incision is done in the uterine wall, most commonly a low transverse incision. The amniotic sac is then ruptured, followed by suctioning of the amniotic fluid and inspection of its color, odor and quantity.
When the infant’s head is delivered, the nose and mouth are suctioned to decrease aspiration of amniotic fluid. The umbilical cord is clamped and cut as soon as the rest of the infant is delivered, and then the baby is handed to members of the neonatal team for immediate assessment and care. Then the placenta is extracted manually, at which time antibiotics are administered to reduce the risk of infection, as well as oxytocin to help contract the uterus and control bleeding. The uterine and abdominal cavities are then inspected and rinsed with saline before incisions are stitched and stapled closed. Finally, the uterine fundus is massaged, blood clots are removed from the vagina as needed, an abdominal dressing applied to the incision, and a pad is applied to the perineum.
Now let’s switch gears and look at the complications of a cesarean birth. The most common maternal complications involve infection, wound dehiscence, hemorrhage, and venous thromboembolism. Other complications include those associated with the procedure, like drug reactions, aspiration pneumonia, as well as injury to the bowel or bladder. Fetal complications, on the other hand, involve unintended preterm delivery, and injuries such as lacerations, fractures, and bruising. Okay, let’s move on to the nursing care you’ll be providing for a client having a cesarean birth. Your primary goals will be to prepare the client for surgery, provide postoperative care, and provide emotional support.